Drowning. "Pale" drowning Drowning in fresh water may cause
Signs of true drowning:
- cyanosis facial skin,
- swelling of the vessels of the neck,
Turn on the stomach, clean the mouth and press on the root of the tongue.
If there is a gag reflex, continue removing water from the stomach (up to 2-3 minutes).
If there is no gag reflex, make sure that there is no pulse on the carotid artery and proceed to resuscitation.
If there is a pulse on the carotid artery, but there is no consciousness for more than 4 minutes, turn on the stomach and apply cold to the head.
In cases of shortness of breath, bubbling breathing - seat the victim, apply heat to the feet, apply tourniquets on the thigh for 20-30 minutes.
Attention! In the case of true drowning, death can occur in the next few hours from repeated cardiac arrest, pulmonary edema, and cerebral edema. Therefore, in each case of drowning, rescue services are necessarily called, and the rescued person must be delivered to the hospital. .
Actions in case of pale drowning
Signs of pale drowning:
- lack of consciousness
- lack of pulse on the carotid artery,
- pallor of the skin,
- sometimes "dry" foam from the mouth,
- more common after falling into icy water.
Move the victim to a safe distance from the hole.
Check for a pulse on the carotid artery.
If there is no pulse on the carotid artery, start resuscitation.
If there are signs of life, transfer the rescued to a warm room, change into dry clothes, give a warm drink.
Attention! In the case of pale drowning, it is unacceptable to waste time removing water from the stomach.
Actions in case of the first stage of hypothermia
Signs of the first stage of hypothermia:
- blue lips and tip of the nose,
- chills, muscle tremors, goosebumps,
- Profuse frothy discharge from the mouth and nose.
If possible, wear additional warm clothing. Force to move.
Give 50-100 ml of wine or other sweet alcohol, provided that within 30 minutes the victim will be taken to a warm room and his mouth did not smell of alcohol .
Attention! The first stage of hypothermia is protective and not life-threatening. It is enough to use additional warm clothes, make them move and take warm food or sweets in order to prevent the onset of a more dangerous stage of hypothermia.
If, after removing from the hole, there is no supply of dry clothes and the ability to make a fire, if possible, lay any paper between the body and wet clothes and continue moving towards the settlement. After 5-7 minutes, the paper will begin to dry out and become a good heat insulator.
Actions in case of the second and third stages of hypothermia
Signs of the second and third stages hypothermia (as they appear):
skin blanching,
Loss of feeling cold and feeling comfortable in the cold,
Complacency and euphoria or unmotivated aggression,
Loss of self-control and adequate attitude to danger,
The appearance of sound, and more often visual hallucinations,
Lethargy, lethargy, apathy,
Oppression of consciousness and death.
Offer warm sweet drink, warm food, sweets.
Take to a warm place as soon as possible.
If there are no signs of frostbite on the extremities, remove clothing and place in a bath of warm water or cover with plenty of heating pads.
Attention! Before immersing the victim in water, be sure to check its temperature with your elbow.
After the warming bath, put on dry clothes, cover with a warm blanket and continue to give warm sweet drinks until the arrival of the medical staff.
Attention! It is unacceptable to offer alcohol to the victim lying in the water.
Related information:
- A) This is what determines, stimulates, induces a person to perform any action included in the activity
Article content: classList.toggle()">expand
How to rescue a drowning person? How effective are pre-hospital resuscitation actions? What should be done after providing first aid before the arrival of doctors? You will read about this and much more in our article.
Almost always, the correct provision of first aid to a drowning person saves the life of the victim, since a professional medical team will not have time to arrive at the scene on time, even if it was called immediately after the formation of such a situation.
How to pull the victim to the shore?
It should be noted that an important element of the potential rescue of a drowning person, if he has not yet had time to dive under water for a long period of time, is his correct pulling out, which provides not only the possibility of resuscitation of the victim, but also the safety of the helper.
The basic scheme for rescuing a drowning person:
First aid for a drowning person
After the victim was brought ashore, it is necessary to proceed with the necessary resuscitation actions.
Algorithm of first aid for drowning (briefly by points):
- from liquid or foreign matter. The victim's mouth opens, dentures, vomit, mud, and liquid are removed from it. When drowning directly in the water, the rescuer lays the person on his stomach on his knee, face down, to allow the liquid to flow freely. Two fingers are placed in the victim's mouth and pressure is applied to the root of the tongue to induce vomiting, which helps to free the airways and stomach from water that has not had time to be absorbed;
- Active pre-resuscitation actions. As part of the implementation of first aid, it is necessary to continue inducing vomiting in the victim in the initial position from 1 point until a cough appears. If this process does not give an effect, then in the vast majority of cases there is no free fluid in the respiratory tract and stomach, since it has managed to be absorbed;
- immediate resuscitation. The victim is turned over on his back and placed in a horizontal position, after which the rescuer proceeds to massage the heart and artificial respiration.
How to provide first aid for drowning, see the video:
With true (wet) drowning
How to provide first aid to a drowning person? As part of the provision of first aid when rescuing a drowning person, when the incident occurred directly within the reservoir and in the human body got a large number of water, the above-described activities are carried out.
Their average duration takes from 2 to 3 minutes for the primary two stages. At the same time, artificial respiration and indirect heart massage are effective for an average of 6-8 minutes. After 10 minutes and the absence of any signs of heartbeat and breathing, with a high degree of probability it is impossible to save a person.
ithealthy
know!
An important factor in true drowning is also the circumstances of the incident. So in salt water, a person's chances of surviving in the absence of breathing and heartbeat are higher, since irreversible processes occur later than in the case of flooding. fresh water- It is possible to restore vital processes within 10-15 minutes.
In addition, the temperature of the water also makes a certain contribution. When drowning in a cold or icy liquid, irreversible destruction processes slow down significantly. In some cases, resuscitation practice recorded situations when a person was brought back to life by carrying out indirect massage heart and artificial respiration 20 and sometimes 30 minutes after drowning.
With asphyxial (dry) drowning
Asphyxic or dry drowning is a pathological circumstance that is formed as a result of spasm of the glottis and suffocation, when water does not penetrate into the respiratory tract.
In general, this type of incident is considered more favorable in the context of the potential for human resuscitation.
What to do with dry drowning? First aid for dry drowning generally coincides with first aid, as for classical drowning, however, the second stage (attempts to induce vomiting and free the airways with the stomach from the accumulated fluid) is skipped and direct resuscitation is immediately applied to the victim.
Resuscitation actions
As part of the resuscitation efforts to provide emergency care when drowning is of a manual nature, two main procedures are performed - this is an indirect heart massage and artificial respiration. The basic rules for helping a drowning person are presented below.
Artificial respiration
The victim is laid on his back, the airway opens as wide as possible, any foreign objects that make it difficult to breathe are removed from the oral cavity. If there is an air duct of a medical design, it must be used as part of the first aid for a drowning person.
The lifeguard takes a deep breath and exhales air oral cavity the victim, covering the wings of his nose with his fingers and supporting his chin, tightly pressing his lips to the victim's mouth. As part of forced ventilation, a person's chest should rise.

The average blowing time is about 2 seconds, followed by a 4 second pause for a slow reflex lowering of the drowned chest. Artificial respiration during drowning is repeated regularly until stable signs of breathing appear or the ambulance arrives.
Indirect cardiac massage
Measures to start cardiac activity can be combined with the implementation of artificial respiration as part of their alternate shift. To begin with, you must first strike with a fist in the area of \u200b\u200bthe projection of the heart- it should be of medium strength, but sharp and fast enough. In some cases, this helps to instantly start the functioning of the heart.

If there is no effect, you need to count two fingers down from the sternum to the center of the chest, straighten your arms, putting one palm on the other, orient yourself to the connection of the lower ribs with the sternum, and then apply pressure strictly perpendicular to the heart with both hands. The heart itself is compressed between the sternum and the spine. The main efforts are carried out with the whole torso, and not just with the hands.
The average depth of indentation should not exceed 5 cm, while the approximate frequency of pressure is about 100 manipulations per minute, in cycles of 30 times with a combination of ventilation of the lungs.
The general cycle, therefore, is as follows: 2 seconds of inhalation of air into the victim, 4 seconds for his spontaneous exit, 30 massage manipulations in the region of the heart and a repetition of the cyclic double procedure.
First aid for children
It is worth noting that the chances of resuscitating a child during drowning are significantly less than an adult, since irreversible processes leading to death develop much faster in him.
On average, there are about 5 minutes to try and rescue a drowned toddler.
Algorithm of actions for providing first aid for drowning a child:
- Pulling the victim to the shore. It is carried out as quickly as possible, while observing the general precautions described earlier;
- Release of the upper airways from foreign substances. You should open the child's mouth, try to free him from any kind of foreign matter, including water, then put a knee and put the baby on his stomach, simultaneously causing the latter to have a gag reflex by pressing on the root of the tongue. The event is repeated until the child has an active cough, and water, along with vomit, stops actively flowing out;
- resuscitation activities. In the absence of the effect of the procedure from the previous paragraph, or if there are signs of a “dry” type of drowning, the child is turned over on his back, placed in a horizontal position, and he is given an indirect heart massage, as well as artificial respiration.
Further rescue actions
If the victim managed to start the breathing of the heartbeat, then he is laid on his side, while continuing to remain in a horizontal position. A person is covered with a blanket or towel for warming, while his condition is constantly monitored and in the event of a repeated stoppage of breathing or heartbeat, manual resuscitation is resumed.
It should be understood that regardless of the circumstances, even if the person is in a satisfactory condition, it is necessary to wait for the arrival of the ambulance team, which will provide the first medical care when drowning. Specialists will competently assess the potential risks for the victim and decide on the need or absence of such hospitalization.
In some cases, the ingress of a significant amount of water into the lungs, secondary cerebral edema and other symptoms appear after a certain period of time, there are no medium-term health effects only when more than 5 days have occurred after drowning, while no pathological symptoms have appeared in a person.
Types of drowning
In general modern medicine distinguishes three types of drowning:
- True drowning. The main sign of such an incident is the ingress of a large amount of water into the lungs and stomach, against which there is swelling of the corresponding tissues and irreversible destruction of their structure. Occurs in every one of the 5 reported cases;
- Asphyxial drowning. It can also occur on water, but the liquid itself does not penetrate into the lungs of the stomach, because before this process a pronounced spasm of the vocal cords is formed with a complete stop of respiratory activity. All basic pathological processes are associated with direct suffocation and shock. Occurs in 40 percent of cases;
- Syncopal drowning. It is characterized by a reflex cardiac arrest, in the vast majority it causes an almost instantaneous death. Occurs in 10 percent of cases;
- Mixed drowning. It has signs of both classic "wet" and asphyxic drowning. Diagnosed in an average of 15 percent of the victims.
The difference between sea and fresh water
Classical medicine distinguishes between drowning in fresh water and sea water according to a number of characteristics:
- Fresh water. There is a stretching of the alveoli and the penetration of the corresponding fluid into the bloodstream by direct diffusion through the violation of the integrity of the alveolar-capillary membrane. Hypotonic hyperhydration develops sharply, the functioning of the blood flow is disrupted.
Due to the absorption of hypotonic waters into the vascular bed, pulmonary edema, hypervolemia, hyperosmolarity, blood thinning with an increase in its volume are formed.
Ventricular fibrillation occurs, unable to cope with a large amount of "diluted" biological fluid. In general, irreversible damage occurs quickly;
- Salty water. The fluid enters the alveoli, which leads to hypertensive dehydration, an increase in the amount of sodium, potassium, magnesium and calcium, as well as chlorine in the blood plasma. In fact, it is not liquefaction that occurs, but, on the contrary, blood thickening, while irreversible damage to the body occurs more slowly compared to fresh water (up to 25 percent).
The processes described above are often separated into separate categories of descriptive characteristics of the medical literature of the 20th century.
Current large-scale studies show that the pathogenesis of drowning in fresh and salt water does not differ significantly in the context of clinical hazard.
Accordingly, the difference in potential resuscitation is actually negligible and amounts to only a few minutes. As real practice shows, the chances of restoring brain function and vital signs are significantly increased cases of drowning with very low temperatures especially in small children.
Individual doctors recorded cases of complete resumption of life 30 minutes after drowning, while all the time the victim had no breathing and heartbeat.
Table of contents of the subject "Acute Respiratory Failure (ARF) with Obstruction of the Airways. Foreign Bodies of the Upper Respiratory Tracts. Pulmonary Embolism (PE).":1. Acute respiratory failure (ARF) with airway obstruction. Laryngospasm. Causes (etiology), pathogenesis of laryngospasm. Emergency care for laryngospasm.
2. Bronchiospasm (bronchial asthma). Causes (etiology), pathogenesis of bronchiolospasm. Emergency care for bronchiolospasm (bronchial asthma).
3. Asthmatic condition. Asthmatic status. Causes (etiology), pathogenesis of status asthmaticus. Stages of status asthmaticus.
4. Principles of treatment of status asthmaticus. Treatment of status asthmaticus stage 1.
5. Treatment of asthmatic status 3 (third) stage. Signs of relief of status asthmaticus. hospitalization issues.
6. Foreign body. Foreign bodies in the upper respiratory tract. Emergency care for foreign bodies.
7. Drowning. True (wet) drowning. Asphyxic (dry) drowning. Syncope type of drowning (death in water). Emergency aid for drowning.
8. Thromboembolism of the pulmonary artery (TELA). Etiology (causes) of thromboembolism. Pathogenesis of pulmonary embolism (PE).
9. Anatomical variants of pulmonary embolism (PE) by localization. Clinical forms of PE. Clinic of pulmonary embolism (TELA).
10. ECG (ecg, electrocardiogram) of pulmonary embolism (PE). X-ray data of TELA. Principles of intensive care for pulmonary embolism (PE). Urgent care.
Drowning. True (wet) drowning. Asphyxic (dry) drowning. Syncope type of drowning (death in water). Emergency aid for drowning.
Drowning- acute pathological condition, which develops during accidental or deliberate immersion in a liquid, with the subsequent development of signs of ARF and AHF, the cause of which is the ingress of liquid into the respiratory tract.
Distinguish 3 types of drowning in water:
1. True (wet).
2. Asphyxia (dry).
3. Death in water (syncope type of drowning).
Etiology. True drowning. It is based on the ingress of water into the alveoli. Depending on the water in which drowning occurred (fresh or sea), there will be a different pathogenesis. Fresh water, due to the difference in the osmotic gradient with blood, quickly leaves the alveoli and enters the vascular bed (see Fig. 10a). This leads to an increase in BCC and hemodilution, pulmonary edema, hemolysis of erythrocytes, a decrease in the concentration of sodium, chloride and calcium ions in plasma, as well as plasma proteins. When drowning in sea water, as a result of the difference in the osmotic gradient between blood and sea water, and here there is a clear predominance of the sea water gradient over blood, part of the plasma leaves the vascular bed. In this regard, the mass of circulating blood decreases (up to 45 ml / kg), the hematocrit increases (V. A. Negovsky, 1977).
Rice. ten. The pathogenesis of drowning in fresh (a) and sea (b) water.Asphyxial drowning occurs without aspiration of water. The basis of this pathology is reflex laryngospasm. The glottis does not allow water to pass through, but it also does not allow air to pass through. Death comes from mechanical asphyxia.
Syncope type of drowning (death in water) occurs as a result of reflex cardiac arrest and respiration. The most common variant of this type of drowning occurs when the victim is suddenly immersed in cold water.
Clinic. At true drowning distinguish 3 periods: initial, agonal and clinical death. The state of consciousness depends on the period of drowning and its type. Respiratory failure is possible from noisy to atonal. There is cyanosis, chills, goose bumps. When drowning in fresh water, there is a clinic of pulmonary edema, arterial and venous hypertension, tachycardia, arrhythmia. From the upper respiratory tract, foam, sometimes with a pink tinge, may be released as a result of hemolysis of red blood cells. When drowning in sea water, arterial hypotension and bradycardia are more characteristic.
Urgent care. Regardless of the water in which drowning occurred, when breathing and cardiac activity stop, the victim needs to carry out a set of resuscitation measures. Before performing artificial respiration, the upper respiratory tract (URT) should be freed from water and foreign bodies(river sand, algae, silt, etc.). The best way to release the upper respiratory tract, especially in children, is to lift the victim by the legs. If it is impossible to perform this manual, it is recommended to lay the victim on the bent knee of the person providing resuscitation assistance and wait for the fluid to flow out of the upper respiratory tract (see Fig. 11). This procedure should take no more than 5-10 seconds, after which it is necessary to proceed to resuscitation.

Treatment in a hospital setting is syndromic in nature and consists of the following areas:
1. Carrying out a complex of resuscitation measures and transferring the patient to mechanical ventilation (according to indications).
2. Sanitation of the tracheobronchial tree, therapy of bronchiolospasm, pulmonary edema.
3. Cupping OSSN.
4. Correction of acid-base balance and electrolytes.
5. Prevention of pneumonia and renal failure.
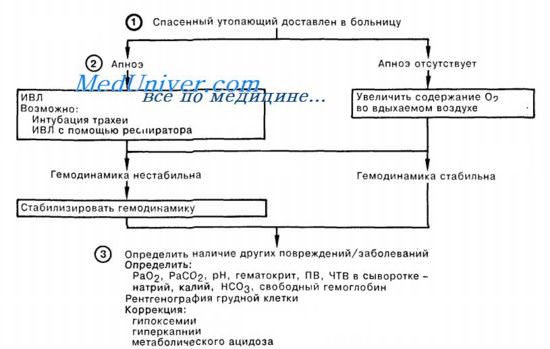
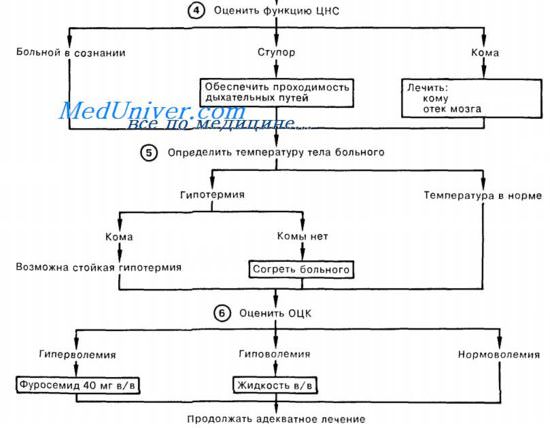
First aid video for drowning patient
Drowning first aid scheme
There are three types of drowning: primary (true, or "wet"), as-
fixed ("dry") and secondary. In addition, in case of accident
there may be death in the water, not caused by drowning (trauma, heart attack
myocardium, disorder cerebral circulation etc.).
Primary drowning is the most common (75-95% of all accidents)
cases in water). It causes fluid to be aspirated into the respiratory
paths and lungs, and then its entry into the blood.
When drowning in fresh water, severe hemodilution quickly occurs.
and hypervolemia, hemolysis develops, hyperkalemia, hypoproteinemia, hy-
ponatremia, a decrease in the concentration of calcium and chlorine ions in plasma. Ha-
rakterna sharp arterial hypoxemia. After removing the victim
from water and first aid, pulmonary edema often develops with
secretion of bloody foam from the respiratory tract.
When drowning in sea water, which is hypertonic in relation to
blood plasma, hypovolemia develops, hypernatremia, hypercalcemia,
hyperchloremia, there is a thickening of the blood. For true drowning in the sea
which water is characterized by the rapid development of edema with secretion from the respiratory
paths of white, resistant, "fluffy" foam.
Asphyxial drowning occurs in 5-20% of all cases. With him
reflex laryngospasm develops and water aspiration does not occur, but
asphyxia occurs. Asphyxial drowning occurs more often in children and
women, as well as if the victim gets into a contaminated, chlorinated
water. In this case, water in large quantities enters the stomach. Maybe
develop pulmonary edema, but not hemorrhagic.
Secondary drowning develops as a result of cardiac arrest
due to the victim getting into cold water ("ice shock",
"immersion syndrome"), a reflex reaction to the ingress of water into the respiratory
paths or middle ear cavity with a damaged tympanic
ponque. Secondary drowning is characterized by a pronounced spasm of the peripheral
some vessels. Pulmonary edema usually does not occur.
Symptoms. The condition of the victims extracted from the water is largely determined by
is divided by the duration of stay under water and the type of drowning, the presence
mental trauma and cooling. In mild cases, consciousness may be
preserved, but the patients are agitated, trembling, frequent vomiting is noted. At
relatively long true or asphyxic drowning consciousness
tanno or absent, sharp motor excitation, convulsions. Dermal
covers are cyanotic. For secondary drowning, a sharp pallor is characteristic
skin covers. The pupils are usually dilated. breath bubbling,
frequent or with prolonged stay under water rare with participation
accessory muscles. When drowning in sea water, edema quickly increases
lungs. Severe tachycardia, sometimes extrasystole. With long and
secondary drowning, the victim can be removed from the water without recognition
respiration and cardiac activity.
Complications. With true drowning in fresh water, already at the end of the first
hours, sometimes later, hematuria develops. Pneumonia and atelectasis
which can develop very quickly, at the end of the first day after drowning
With severe hemolysis, hemoglobinuric nephrosis and
acute renal failure.
Urgent care. The victim is removed from the water. With loss of consciousness
artificial ventilation the easy way mouth to nose preferably
start on the water, but these techniques can only be performed by a well-prepared
tovlenny, physically strong rescuer. artificial lung ventilation
carried out as follows: the rescuer holds his right hand under the right
howl with the victim's hand, being behind his back and to the side. His right
with the palm of the hand, the rescuer closes the mouth of the victim, at the same time pulling
up and forward his chin. The blowing of air produces in the nasal passages
dy drowned.
When removing the victim to a boat, lifeboat or shore
it is necessary to continue artificial respiration, for this purpose it is possible to use
use an airway or mouth-to-nose mask and Ruben bag. When from-
the absence of a pulse carotid arteries should immediately begin indirect
heart massage. It is a mistake to try to remove "all" the water from the lungs.
With true drowning, the patient is quickly laid with his stomach on the thigh
the rescuer's leg of the rescuer and with sharp jerky movements compress the sides
chest surfaces (within 1015 s), after which again
bring him back. The oral cavity is cleaned with a finger wrapped in a handkerchief
or gauze. If trismus of masticatory muscles has come, you should press
fingers on the corners of the lower jaw. If there is an electrical or
foot suction to clean the mouth, you can use a rubber
teter of large diameter, but with pulmonary edema, one should not strive to
remove foam from the respiratory tract, as this will only increase swelling.
When carrying out artificial ventilation of the lungs by methods from the mouth to
mouth or from mouth to nose, one condition is absolutely necessary:
the patient's head should be in the position of maximum occipital extension
banya. Rescuer, being on the side of the victim, with one hand
holds his head in an unbent position, pressing his palm on his forehead,
and with the other hand slightly opens his mouth by the chin. At the same time, I do not follow
em bring forward lower jaw, since with the correct position of the go-
catches the patient's tongue root and epiglottis is displaced anteriorly and opens
air access to the larynx. The rescuer takes a deep breath and, cuddling up
with his lips to the mouth of the patient, makes a sharp exhalation. This is followed by 1 and
II with the fingers of the hand placed on the forehead, squeeze the wings of the nose to prevent
blocking the exit of air through the nasal passages. If you open the patient's mouth
it is possible or the oral cavity is not freed from the contents, to blow in air
can be through the nose of the victim, covering his mouth with his palm. The rhythm is artificial
leg breathing 12-16 in 1 min.
In some cases, the respiratory tract of a drowned person may not be
passable due to the presence of a large foreign body in the larynx or persistent
laryngospasm. In this case, a tracheostomy is indicated, and in the absence of
necessary conditions and tools - conicotomy.
After the patient has been delivered to the rescue station, resuscitation measures
riyatiya must be continued. One of the most common mistakes is
premature termination of artificial respiration. The presence of the victims
greater respiratory movements, as a rule, do not indicate recovery
lesion of full ventilation of the lungs, so if the patient does not have
consciousness or pulmonary edema has developed, it is necessary to continue artificial
breath. Artificial respiration is also necessary if
the victim has respiratory rhythm disturbances, increased breathing more than 40
in 1 min, sharp cyanosis.
With saved breathing, inhalation of ammonia vapors should be carried out.
alcohol (10% ammonia solution).
In case of chills, rub thoroughly skin, wrap
injured person in warm dry blankets. Heating pads are contraindicated
if consciousness is absent or impaired.
With respiratory disorders and pulmonary edema, tracheal intubation and
artificial ventilation of the lungs, preferably 100% oxygen
house. Intubation can be done by intravenous
muscle relaxants (listenone - 100-150 mg) with a preliminary introduction of 0.1%
atropine solution - 0.8 ml. With a sharp excitation of the patient, atropine and
listenone can be injected into the root of the tongue. In the presence of a respirator type RO,
"Phase", "Lada" output resistance +8 is shown; +15 cm aq. Art. under
BP control.
Particular emphasis should be placed on the danger of premature termination of the
artificial lung ventilation. The appearance of spontaneous respiratory
movements does not mean the restoration of an adequate pulmonary valve
tion, especially in conditions of pulmonary edema.
After tracheal intubation and initiation of artificial respiration,
insert a probe into the stomach and evacuate the water accumulated in it and stagnant
content.
When drowning in fresh water to the victim in stationary conditions
with severe cyanosis, swelling of the cervical veins, high central venous
pressure shows bloodletting in a volume of 400-500 ml from the central vein
(subclavian or jugular). With severe hemolysis, intravenous
transfusion of 4-8% sodium bicarbonate solution at a dose of 400-600 ml
(under the control of the acid-base state). Against the backdrop of artificial
created metabolic alkalosis, lasix 40-60 mg should be administered
2-3 times a day until the disappearance of gross hematuria.
Concentrated protein transfusion is indicated for hypoproteinemia
(20% albumin - 100-150 ml).
With late development of pulmonary edema, if there are no indications for artificial
ventilation of the lungs, inhalation of oxygen passed through
50% alcohol or antifomsilane. If pulmonary edema develops against the background of arterial
al hypertension, shown intravenous administration ganglionic blockers (ar-
fonad 5% solution - 5 ml or pentamine 5% solution - 0.5-1 ml in 200 ml 5%
glucose solution drip under strict control of blood pressure). It is necessary to
changing large doses of corticosteroids - 800-1000 mg of hydrocorgizone or
150-180 mg of prednisolone per day. Previous use of antibiotics
for the prevention of aspiration pneumonia. To combat motor
arousal and to protect the brain (prevention of hypoxic encephalopathy)
ii) shows intravenous administration of sodium hydroxybutyrate - 120-150 mg / kg
or neuroleptanalgesics - 0.3-0.7 mg of menthanil with 12-15 mg of droperidol.
When drowning in sea water, artificial ventilation of the lungs with
living pressure at the end of the exit should be started as early as possible.
Transfusion of protein solutions (plasma, albumin) is shown. Special attention
should be addressed to the elimination of hypovolemia and correction of rheological
blood properties. Intravenous transfusion of rheopolyglucin is indicated, previously
the use of heparin - 20000-30000 IU / day.
The rest of the therapy is carried out according to the principles described above.
Hospitalization. At severe forms drowning the victim is necessary
transport not to the nearest hospital, but to a well-equipped department
resuscitation institute. During transportation, you must continue to use
artificial ventilation of the lungs and all other necessary measures. Beli
was introduced gastric tube, during transportation it is not removed.
If for some reason the tracheal intuation was not performed, trans-
it is necessary to port the victim on his side with the headrest lowered
Drowning- this is the closure of the respiratory openings of the mouth and nose by immersing the face in a liquid or semi-liquid medium, causing the closure of the airways or reflex closure (spasm) of the glottis, accompanied by a violation or cessation external respiration and causing death by strangulation.
Drowning can occur while swimming in fresh and salt water, in various reservoirs, rivers, lakes, sea, bath, when falling into a puddle, liquid mud, falling into various containers filled with technical or food liquids, semi-liquid masses, sewage.
Drowning contribute to intoxication, overwork, hypothermia, increased sweating, overheating of the body, overflow of the stomach with food, a sharp change in the conditions of blood circulation in water, an increase in the load on the cardiovascular system, mental factors, diseases of the cardiovascular and nervous systems, injuries.
Bathing in cold water or prolonged exposure to relatively warm water can lead to convulsive contraction of certain muscle groups. Such a reaction occurs during prolonged swimming in one style, a feeling of fear, panic. Occasionally, the so-called "immersion syndrome" (water, ice or cryogenic shock) occurs due to a sharp temperature drop, causing over-irritation of skin thermoreceptors, vasospasm, cerebral ischemia and reflex cardiac arrest.
Most often, drowning is caused by injuries caused by inept diving, diving in a shallow place, hitting objects on the water, in the water and at the bottom. Sometimes there are damages by details of water transport. Extremely rarely observed damage caused by sharp tools and firearms.
Sudden and rapid immersion of a person in water, depending on the low water temperature compared to the body and the surrounding air, hydrostatic pressure that changes with the depth of immersion, psycho-emotional stress, causes certain changes that determine the type of drowning and the genesis of death.
Drowning can occur in several ways. Among them are: aspiration (true, wet drowning), spastic (asphyctic, dry drowning), reflex (syncope) and mixed types.
Occasionally there is death in the water caused by diseases (myocardial infarction, non-traumatic cerebral hemorrhage), as well as injuries not related to drowning.
The pattern and duration of drowning is affected by a number of conditions, such as water temperature, fresh or salty, speed of the current, waves, cold water training, and the will to live.
The aspiration type is characterized by the filling of the airways and alveoli with fluid and a significant dilution of the blood by the absorbed fluid. This type of drowning proceeds in several phases, like mechanical asphyxia.
At the beginning of a true (wet) drowning, a person is conscious and fights for his life. Trying to escape, thanks to the movements of his arms and legs, he either floats to the surface, then again plunges into the water, screams, calls for help, grabs the surrounding objects.
Plunging into the water, a person instinctively holds his breath (pre-asphyctic period) for a different time, due to the state of health and fitness (about 1 minute), tries to emerge.
On the surface takes convulsive breaths, makes chaotic swimming movements. In connection with the growing lack of oxygen in the body, involuntary respiratory movements appear. The accelerated breathing rate during ascent increases the oxygen consumption of the tissues. Respiratory failure is exacerbated by aspiration of even small amounts of water, coughing in response to irritation of the trachea, and bronchospasm. Then comes a deep breath (inspiration), and water under pressure enters the mouth, nose, larynx, trachea and bronchi, causing irritation of the receptors of their mucous membranes, which is transmitted to the cerebral cortex, where the excitation process occurs. Re-irritation of the mucous membranes leads to the release of a large amount of mucus containing protein, which mixes with water and air during breathing, forming a persistent grayish-white or pinkish foam, stained in this color with an admixture of blood from ruptured blood vessels of the alveoli (inspiratory dyspnea stage).
Taking convulsive breaths while emerging, a person can swallow water. A full stomach makes it difficult for the diaphragm to move. Physical stress and fear further increase oxygen deficiency, which irritates the respiratory center. Involuntary respiratory movements are formed under water (the stage of expiratory dyspnea). Following this reflexively there is a deep exhalation, ejecting from the respiratory tract, along with water, the air contained there. At 3-4 minutes diffuse protective inhibition of the cortex sets in. By this time, consciousness is usually lost, air bubbles appear on the surface of the water and the person sinks to the bottom. In the middle or end of the second minute after immersion in water, general convulsions occur due to the spread of overexcitation processes in the cortex and the capture of the motor zones of the cortex by them, reflexes are lost. The person becomes immobile. Further, the waves of the initial motor excitation begin to descend into the underlying parts of the central nervous system and, reaching the cervical part spinal cord, cause a series of deep, but rare breaths with a wide open mouth (the so-called terminal respiratory movements). Water, swallowed, enters the stomach and the initial section of the small intestine. In the stage of terminal breathing, it enters the airways in a wide stream under pressure that increases with the depth of immersion of the body, filling the bronchi and alveoli. Due to high pulmonary pressure, an expansion of the alveoli develops - alveolar emphysema. Water enters the tissue of the interalveolar septa, breaks the walls of the alveoli, penetrates the lung tissue, displaces the air in the bronchi, and mixes with the air contained in the lungs (normally up to 2.5 liters). Through the capillaries, water enters the vessels of the pulmonary circulation, significantly diluting the blood and hemolyzing it. Blood diluted with water enters the left half of the heart, and then into big circle circulation. There comes a final cessation of breathing, soon the work of the heart stops, and after 5-6 minutes death occurs from a lack of oxygen (Fig. 281).
When examining a corpse in cases of wet drowning, pallor of the skin is observed, which is formed due to spasm of the skin capillaries, goose bumps due to contraction of the muscles that raise the hair, grayish-white or pink persistent fine bubble foam around the respiratory openings of the nose and mouth, described by the Russian scientist Krushevsky in 1870 It occurs as a result of air mixing with a large amount of mucus containing protein released due to irritation of the mucous membrane of the respiratory tract with water. This foam persists for up to 2 days. after removing the corpse from the water, and then dries, forming a film. Its formation is facilitated by the leaching of a surfactant (sulfactant) from the surface of the alveolar epithelium, which ensures the expansion of the alveoli during respiration, which was noticed by the Ukrainian scientist Yu.P. Zinenko in 1970
The presence of foam indicates active respiratory movements in the process of drowning. Due to the rupture of the vessels of the alveoli, the released blood stains the foam in a pinkish color.
The spastic type is caused by persistent reflex laryngospasm, which closes the entrance to the respiratory tract due to irritation of the respiratory tract receptors by water.
This type of drowning is formed at the moment of sudden ingress of water at a temperature of about 20 ° C into the upper respiratory tract. Water irritates the mucous membranes and endings of the upper laryngeal nerve, leads to spasm of the vocal cords and reflex cardiac arrest. The spasm of the vocal cords closes the glottis, which prevents the entry of water into the lungs during immersion and the exit of air from the lungs at the time of resurfacing. The sharply increased intrapulmonary pressure causes acute, accompanied by loss of consciousness, asphyxia. Phases of deep and atonal breathing are manifested by intense movements of the chest. Sometimes a terminal pause may be missing. In connection with the fall in cardiac activity, conditions are created for the development of pulmonary edema, impaired permeability of the alveolar-capillary membranes, which causes the final units of the lungs (alveoli) of blood plasma to enter the air spaces, which, mixing with air, forms a stable fine bubble foam. Edema can also be caused by mechanical damage to the membrane due to a drop in intrapulmonary pressure due to intense false inspiration with a closed glottis.
Sometimes a small amount of fluid enters the airways, which is quickly absorbed, especially in cases of drowning in fresh water, and does not cause blood thinning. On the cut, the lungs are dry, and therefore such drowning is called asphyxial, or dry, or drowning without aspiration of water.
The likelihood of laryngospasm depends on age, body reactivity, sex, water temperature, its contamination with chemical impurities, chlorine, sand, shells and other suspended particles. Most often, laryngospasm is observed in women and children.
During the examination of the corpse, attention is paid to the blue-purple color of the skin, especially in the upper parts of the body, abundant confluent cadaveric spots, hemorrhages in the skin of the face and mucous membrane of the eyelids, dilation of the vessels of the white membrane of the eyes. Occasionally there is a white fine bubble foam around the openings of the nose and mouth.
An internal study reveals a sharp emphysema of the lungs, their fluffiness, multiple petechial hemorrhages under the organ pleura, epicardium, in the mucous membrane of the respiratory and urinary tract, gastrointestinal tract against the background of dilated vessels. Rasskazov-Lukomsky-Paltauf spots are absent. The right ventricle of the heart is filled with blood. Blood in the heart may be in the form of clots, especially in the case of alcohol intoxication. The stomach usually contains a significant amount of watery contents, the internal organs are overflowing with blood.
Sometimes drowning begins as an asphyxial type, and ends as a true drowning, when laryngospasm is resolved by water penetrating the respiratory tract and lungs. It is possible to distinguish true insulation from false by the signs given in Table. 26.

Occasionally, signs of asphyxial and true drowning are absent. Such drowning is called reflex (syncope). This type is associated with rapid reflex respiratory arrest and primary cardiac arrest as a response of the body to the aquatic environment under extreme conditions (water shock, allergic reaction to water, etc.).
It arises from the action of cold water on the body, which increases the spasm of the vessels of the skin and lungs. There is a contraction of the respiratory muscles, resulting in severe violations of breathing and cardiac activity, hypoxia of the brain, leading to the rapid onset of death even before the development of actual drowning. Syncopal type drowned contribute to: emotional shock immediately before immersion in water (shipwreck), hydroshock caused by exposure to very cold water on the skin, laryngopharyngeal shock from the action of water on the receptor fields of the upper respiratory tract, water irritation of the vestibular apparatus in people with a perforated eardrum.
death in the waterrare in practice. As a rule, it is observed in people suffering from diseases of the cardiovascular system (angina pectoris, postinfarction cardiosclerosis, acute coronary and respiratory failure), pulmonary tuberculosispneumosclerosis,diseases of the central nervous system (ecilepsy, mental disorders). The cause of death in water in divers can be pulmonary barotrauma, nitrogen anesthesia, oxygen starvation oxygen poisoning, subarachnoid hemorrhage in diseases of the cerebral vessels, allergic shock to water associated with the effect of an allergen in water on a sensitized organism, fainting followed by a reflex caused by water irritation of the nasopharynx and larynx, leading to drowning, prolonged exposure to water at a temperature of +20 °C, causing progressive heat loss, leading to hypothermia, damage to the tympanic membranes followed by water irritation of the middle ear and reflex cardiac arrest or water entering the middle ear through a perforated tympanic membrane due to a previous disease; irritation of the vestibular apparatus, leading to vomiting and drowning; pathways, aspiration of vomit during the onset of unconsciousness.
An internal study in the tympanic cavities of the middle ear reveals fluid. It enters through the Eustachian tubes or a damaged eardrum. The same fluid is also detected when opening the sinuses of the frontal and basilar bones of the skull. It enters these sinuses due to laryngospasm, which causes a decrease in pressure in the nasopharynx and the flow of water into the pear-shaped cracks. The volume of water in them can reach 5 ml, which was first noticed and described by V.A. Sveshnikov (1965).
Drowning may be accompanied by an outpouring of blood into the tympanic cavities, mastoid cells and caves. It may be in the form of loose accumulations or profuse soaking of the mucous membranes. Their occurrence is associated with an increase in pressure in the nasopharynx, circulatory vascular disorders, which, in combination with pronounced hypoxia, lead to an increase in the permeability vascular walls and outpouring of blood.
AT tympanic cavity there is sand and other foreign particles from the reservoir. Blood outflows into the middle ear and tympanic membrane are revealed.
When examining the corpses of drowned people, bilateral, parallel to the longitudinal fibers, blood bundles of the sternocleidomastoid and pectoralis major muscles (Paltauf), broad and scalene muscles, and neck muscles (Reuters) are found. They occur as a result of strong muscle tension during an attempt to escape from drowning. Occasionally, in the circumference of the nose and mouth and in their openings, vomit is found, indicating vomiting in the agonal period.
The mucous membrane of the entrance of the upper respiratory tract is reddened, swollen, sometimes with pinpoint hemorrhages, which is explained by the irritating effect of water.
The same foam, as in the circumference of the mouth and nose, is also detected in the respiratory tract. Sometimes foreign inclusions (sand, algae, silt, small and large stones) are found in it, indicating drowning in a shallow place.
Foreign particles can penetrate into the corpse when they stay and stay in muddy water containing them for a long time, in fast-flowing water bodies, and therefore their evidentiary value is small. Large pebbles, deeply penetrated into the trachea, indicate active aspiration in the convulsive period of drowning. In the respiratory tract, gastric contents are sometimes found, penetrating to the small bronchi. In such cases, it should be noted whether it is squeezed out of the bronchi on the cut. Its presence indicates vomiting in the agonal period. Occasionally, mucus is found in the respiratory tract. Foam in the airways can form as a result of pulmonary edema, during vigorous artificial respiration, mechanical asphyxia from squeezing the neck with a noose or hands, and as a result, prolonged agony. The mucosa of the trachea and bronchi is edematous, cloudy, the foam is usually unstable and large-bubbly.
Lungs - large, completely fill the pleural cavities and sometimes "bulge" out of them, cover the heart, emphysematously swollen, increased in volume and sometimes in weight, which is explained by the penetration of fluid during wet drowning. The edges of the lungs are rounded, go behind each other, sometimes cover the heart bag. On the surface of the lungs, you can see the imprints of the ribs, which appear traps, between which the lung tissue acts in the form of rollers - "the lung of a drowned person." Similar prints are also found on the posterolateral surfaces of the lungs. Such changes are explained by the pressure of water penetrating the respiratory tract into the lungs, on the air present there, which breaks the walls of the alveoli and passes under the pulmonary pleura, causing emphysema. Water enters the place of the displaced air. As a result, the lungs increase significantly in volume, exerting pressure from the inside on chest, as a result of which transverse grooves appear on them - traces of the pressure of the ribs.
An increase in lung volume occurs during vigorous and prolonged artificial respiration, which must be remembered when examining a corpse. The upper lobes and the lung edges adjacent to the root are usually dry and distended with air. The organ pleura is unclear, under it there are rather large spilled reddish-pink spots with indistinct blurry borders, described independently by Rasskazov (1860), Lukomsky (1869), Paltauf (1880) and received the name Rasskazov-Lukomsky-Paltauf spots in the literature. Their color and size are due to the amount of water that has entered the systemic circulation through the ruptured and gaping capillaries of the interalveolar septa, and blood hemolysis, as a result of which diluted and hemolyzed blood becomes lighter, its viscosity decreases, it liquefies, and hemorrhages blur, acquiring fuzzy contours. The lungs become "marble" due to the alternation of protruding pink and sinking red areas. Drowning in sea water does not cause hemolysis, and they retain their normal color.
To the touch, light doughy, reminiscent of a sponge soaked in water. In wet drowning, the lungs are huge, with alternating dry areas with watery ones, and acquire a gelatinous appearance. A foamy fluid, similar to that contained in the respiratory tract, flows from the cut surface of such lungs. The lungs are heavy, full-blooded, with hemorrhages under the pulmonary pleura.
In cases of dry drowning, the lungs are emphysematously swollen, dry, under the pulmonary pleura, the mucous membrane of the gastrointestinal tract, renal pelvis, Bladder- Tardieu spots that form during inspiratory dyspnea. In the initial parts of the respiratory tract, there may be particles of silt, etc. The venous system is full of blood with a small amount of dark red clots.
From drowning in sea water, which is a hypertonic medium in relation to blood, blood plasma escapes into the alveoli, which leads to the rapid onset of pulmonary edema and pulmonary insufficiency. The blood does not liquefy, its viscosity increases, there is no hemolysis of erythrocytes, Rasskazov-Lukomsky-Paltauf spots are not observed. Areas of atelectasis are combined with foci of emphysema and uneven blood supply.
Liquefaction of the blood contained in the cavity of the left ventricle is a consequence of intravascular hemolysis and is a valuable sign that occurs only in true drowning in fresh water, which quickly permeates the endocardium of the left ventricle and aortic intima.
Examining the corpses of the drowned, F.I. Shkaravsky drew attention to the swelling of the liver, bed and walls of the gallbladder of drowned people.
As a result of congestion and an increase in the volume of fluid in the bloodstream, the volume and mass of the liver increase.
The section draws attention to a large amount of fluid in the stomach, sometimes with an admixture of silt, sand, aquatic plants that penetrate into the stomach when swallowed during drowning. The same fluid is found in duodenum, where it passes only through the in vivo open pylorus as a result of increased reflex peristalsis, which can be considered a sign of drowning.
The overflow of the stomach with swallowed water, especially sea and polluted, causes vomiting. On the gastric mucosa, there are banded hemorrhages, as well as ruptures in the region of the lesser curvature, which are the result of vomiting in the agonal period or hitting the stomach with water. Occasionally, petechial hemorrhages occur under the pancreatic capsule.
The signs of a corpse being in the water, accompanying signs of drowning, include: wet clothes covered with silt, sand with the presence of shells, fish, crayfish, water bugs, algae and fungi in its folds, characteristic of this reservoir, sticky hair, sharp pallor of the skin, raised vellus hair (“goosebumps”), wrinkling of the pectoral nipples, areola of the breast and mammary glands, scrotum, glans penis, pink color of the skin at the edges of cadaveric spots, rapid cooling of the corpse, skin maceration phenomena, “bath hand”, “skin laundresses”, “glove of death”, “sleek hand”, post-mortem hair loss, rapid development of decay, fat wax, post-mortem injuries.
A sharp pallor of the skin is formed when immersed in cold - below body temperature - water, which causes contraction of the vessels of the skin and the pallor of its integument.
The pink color of the skin along the edges of cadaveric spots occurs due to swelling and loosening of the epidermis under the influence of water. This facilitates the penetration of oxygen through the skin, which oxidizes hemoglobin and converts it into oxyhemoglobin.
The pink color of the skin is also observed on the surface of the skin, free from cadaveric spots, if the body is removed from cold water, which was noticed by E. Hoffman and A.S. Ignatovsky.
"Goose skin" is formed under the influence of cold water or only cold on the skin, and in some disorders of the nervous system - due to contraction of smooth muscles.
The surface of the skin is covered with multiple tubercles, the formation of which is due to the contraction of smooth muscle fibers connecting the surface layers of the skin with the hair follicles. As a result of this, they raise them to the free surface of the skin, forming small tubercles in the places where the hairs exit.
Irritation of the skin with water leads to a contraction of the muscle fibers of the pectoral nipples, areola circles of the breast, scrotum, as a result of which their contraction occurs 1 hour after being in the water.
A significant influence on their development is the temperature of the environment, air, the depth of the reservoir, the concentration of salts in the environment (fresh or salty), the mobility of water (stagnant or flowing), the speed of the flow, the thermal conductivity of the medium, clothing, gloves and shoes.
Maceration is one of the signs of a corpse being in the water. Maceration, or softening, is formed under the action of water, as a result of which the epidermis soaks, swells, wrinkles and gradually exfoliates on the palms and soles. Maceration is well detected in places where the skin is thick, rough, callused. It starts with the hands and feet. First, whitening and fine folding of the skin appears (weakly pronounced maceration, “bath skin”), then pearl-white color and large folding of the skin (clearly pronounced signs of maceration - “washerwoman’s skin”. Gradually, the epidermis is completely separated along with the nails (sharply pronounced signs of maceration).The skin is removed along with the nails (the so-called "glove of death"). After its departure, it remains devoid of the epidermis, smooth skin("sleek hand").
In the future, maceration extends to the entire body.
In warm running water, maceration is accelerated. Cold water, gloves and shoes hold her back. The degree of development of maceration makes it possible to roughly judge how long the corpse has been in the water. The literature presents various terms for the appearance of initial and final signs of maceration without regard to water temperature. The most complete timing of the development of skin maceration depending on the water temperature was studied by Ukrainian scientists E.L. Tunina (1950), S.P. Didkovskaya (1959), supplemented by I.A. Kontsevich (1988) and are presented in Table. 27.

Due to loosening of the skin after about 2 weeks. hair loss begins and by the end of the month, especially in warm water, complete baldness occurs. In places of fallen hair, their holes are clearly visible.
The presence of original lubrication protects the skin of newborns from maceration. The first signs of it appear by the end of 3-4 days, and the complete separation of the epidermis - by the end of the 2nd day. months summer and for 5-6 months. in winter.
A drowned person sinks to the bottom and at first, if there is no strong current, he remains in place, but rotting develops and the corpse floats up.
Putrefactive changes begin to develop from the intestines, then the corpse floats up if there are no mechanical obstacles. The lifting force of putrefactive gases is so great that a load weighing 30 kg with a total weight of 60-70 kg is not an obstacle to ascent.
D.P. Kosorotov (1914) gives an example when a ship with 30 bulls in the hold sank in the ocean off the coast of India. All efforts to raise it from the water were in vain, but a few days later the ship surfaced due to the development of putrefactive gases in the corpses of oxen.
In warm water, decay processes develop faster than in cold water. In small reservoirs with a water temperature of more than 22 ° C, the corpse may float up as early as the second day. AT middle lane Russian corpses float on the second or third day, depending on the temperature of the water. According to the Japanese researcher Furuno, from July to September, in cases of drowning at a depth of 1-2 m, the corpse emerges after 14-24 hours, at a depth of 4-5 m - after 1-2 days, at a depth of 30 m - after 3-4 days . In winter, corpses can stay in the water for up to several months. Rotting in water occurs more slowly than in air, but after extraction from water, putrefactive processes proceed extremely rapidly. Already 1-2 hours after the removal of the corpse, the skin takes on a greenish color, cadaveric emphysema develops, the corpse begins to swell, the skin acquires a dirty green color, a putrefactive venous network and blisters appear. A fetid odor emanates from the corpse. In corpses that are in the water in summer 18 hours and in winter 24-48 hours, along with whitening of the hands and feet, the light blue color of the skin turns into a brick-red color of the head and face up to the ears and the upper part of the occipital region. The head, neck and chest acquire a dirty green color interspersed with dark red in summer after 3-5 weeks, in winter - after 2-3 months After 5-6 weeks. summer and winter more than 3 months the body swells with gases, the epidermis exfoliates everywhere, the entire surface takes on a gray or dark green color with a putrid venous network. The face becomes unrecognizable, the color of the eyes is indistinguishable. Determination of the time spent by the corpse in the water becomes impossible in the summer after 7-10 weeks. and in winter after 4-6 months due to the development of putrefactive changes. If something interferes with the ascent, then the decay that has begun is suspended and the formation of a fat wax gradually occurs.
Occasionally, corpses removed from the water are covered with algae or fungi. In corpses that are in running water, fluffy algae in the form of scattered hairy areas are found on the 6th day, on the 11th day they are the size of a walnut, on the 18th day the corpse is dressed as if in a coat of algae, which after 28- 30 days fall off, after which on the 8th day a new growth follows, having the same course.
In addition to these algae, after 10-12 days, mucus-like fungi appear in the form of small red or blue circles with a diameter of 0.2-0.4 cm.
The presence of a corpse in water is judged by the presence of fluid in the tympanic cavity of the middle ear, in the sinuses of the main bone (symptom of V.A. Sveshnikov), fluid in the respiratory tract, esophagus, stomach, small intestine, pleural (Krushevsky's symptom) and abdominal (Moro's symptom) cavities, plankton in the lungs with the integrity of the skin and in other organs in the presence of damage to it.
Moro in the pleural and abdominal cavities found a blood-colored fluid in an amount of up to 200 ml, which seeped into the pleural cavities from the lungs, and into the abdominal cavity from the stomach and intestines. The age of the corpse in the water can be determined by the flow of fluid into the pleural cavities and the disappearance of signs of drowning. The presence of fluid in the pleural and abdominal cavities indicates that the corpse has been in the water for 6-9 hours.
The enlargement of the lungs during the stay of the corpse in the water gradually disappears by the end of the week. The spots of Rasskazov-Lukomsky-Paltauf disappear after a 2-week stay of the corpse in the water. Tardieu spots are determined on the surface of the lungs and heart up to a month after drowning (Table 28).

Laboratory diagnostics for drowning
Many laboratory methods have been proposed to diagnose drowning. Among them, the most widely used microscopic methods of research - histological method research on diatom plankton and pseudoplankton.
Plankton- the smallest organisms of plant and animal origin, located in tap water, water of various reservoirs, in the air. They are typical for this reservoir and have specific features. In the diagnosis of drowning highest value has phytoplankton, and especially diatoms. Their shell is made of silicon that can withstand the impact high temperatures, strong acids and alkalis. The form of diatoms is diverse and typical for each reservoir.
Plankton, along with water, enters the mouth, from there into the respiratory tract, lungs, of which through the vessels into left heart, aorta and blood vessels spread throughout the body, lingering in the parenchymal organs and bone marrow ge long tubular bones(Fig. 282). Plankton persists for a long time in the axils of the main bone and can be found in scrapings from its walls. Together with water from the lungs, grains of sand suspended in water, starch grains, the so-called pseudoplankton (Fig. 283), can also enter the bloodstream. Until recently, plankton and pseudoplankton detection methods were considered the most convincing methods for diagnosing drowning. Their subsequent check showed the possibility of post-mortem penetration of plankton elements into the lungs and other organs of the corpse with damage to the skin. Therefore, the detection of plankton and pseudoplankton has evidential value only when the skin is intact.
At present, the histological method of studying internal organs has become widespread. The most characteristic changes are established in the lungs and liver. On the section of the lungs, foci of atelectasis and emphysema, multiple ruptures of the interalveolar septa with the formation of so-called spurs facing the inside of the alveoli, focal outpouring of blood into the interstitial tissue, and swelling are revealed. In the lumen of the alveoli are light pink masses with an admixture of a certain amount of erythrocytes.
In the liver, the phenomena of edema, expansion of precapillary spaces with the presence of protein masses in them. The wall of the gallbladder is edematous, the collagen fibers are loosened.
On the corpse of a person found or removed from the water, there may be a variety of injuries. A correct assessment of their morphology and localization will allow you to correctly assess what happened and avoid wasting time searching for non-existent intruders. The main questions that an expert must answer are: who, during what, what and how long ago the damage was done.
The most common damage occurs when diving. They are formed when the jump technique is incorrectly performed, hitting objects in the fall path, objects in the water, hitting the bottom, and objects on it and in it. Impacts on objects in the path of fall, located in the water, and objects at the bottom cause extremely diverse damage, reflecting the characteristics of the contact surfaces and localized in any of the areas of the body, on any of its surfaces, sides, levels (Fig. 284).


Evaluating them, it is necessary to take into account the position of the corpse in the water after death. The human body is somewhat heavier than water in terms of its specific gravity. The presence of a small amount of clothing and gases in the gastrointestinal tract allows the corpse to be known time at the bottom. A significant amount of gases in the gastrointestinal tract and developed during the process of decay quickly raises the corpse from the bottom, and it begins to move under water, and then floats to the surface. Persons in warm clothes sink to the bottom faster. The dressed corpses of men usually float face down, with their heads down, the corpses of women - face up, and the legs weighed down by the dress can be lowered below the head. This situation is explained anatomical structure male and female bodies.
Hit by a stream of water at the time of entry into it sometimes forms ruptures of the eardrum. The ingress of water into the cavity of the middle ear causes a loss of orientation of movements in the water. Those who jump into the water experience ruptures of the eardrum, injuries in the lumbar region, contusions and dislocations of the spine in lumbar due to the bending of the body entering the water, sprains and muscles, depression spinous processes of the vertebrae, fractures of the spine from hitting the water. If you fall into the water incorrectly, there may be bruises and ruptures of internal organs, shock, fractures of tubular bones, dislocation of the shoulder joint.
Rarely, injuries found in victims are not fatal in and of themselves, but can cause a momentary loss of consciousness sufficient to cause drowning.
Hitting the water while entering it flat causes bruises, bruises and damage to internal organs, the severity of which is determined by the angle and height of the fall. A blow to the epigastric region of the abdomen or the vulva sometimes causes shock, leading to death. An incorrectly performed “soldier” jump with legs spread apart causes bruises on the heels, scrotum, testicles, followed by the development of traumatic epididymitis. A swallow jump causes damage to the hands of one or both hands, any of the surfaces of the head, the chin, at the handle of the sternum from a chin strike. Sometimes there are fractures of the base of the skull and spine, accompanied by trauma to the brain and spinal cord, causing paralysis of the limbs, due to the level of damage to the spinal cord.
Drowning in a shallow place is accompanied by the formation of abrasions on the limbs and torso from hitting the bottom and objects on it.
Parts of sea and river vessels cause a variety of damage up to the separation of the body. Rotating propeller blades inflict damage resembling chopped. The presence of several identically directed fan-shaped wounds indicates the action of propeller blades with the same direction of turns.
The significant time spent by the corpse under water in a stagnant reservoir and the developing putrefactive changes do not exclude the possibility of the corpse moving along the bottom and in various layers of water, dragging along the bottom with a blow against various objects in the water and on the surface. In reservoirs with flowing water, the listed damage can form even before the development of putrefactive changes. In mountain rivers and rivers with a fast current, corpses sometimes move a considerable distance. Depending on the topography of the bottom, objects on it and individual stones, rapids, driftwood, clothes and shoes are sometimes completely removed, and on the remaining ones there are various damages caused by friction and hooking. Damage to the corpse, caused by dragging and impact, is localized on the skin, nails and even bones of any of the surfaces of the body. To move with water, transverse ruptures of the legs in the area are typical. knee joints, wear of shoe socks for men and heels for women, abrasions on the back of the hands. Such localization and morphology of injuries is explained by the fact that the corpse of a man floats face down, and women - up. In these cases, cadaveric spots in men are primarily formed and located on the face.
Injuries by the action of sharp objects can be inflicted when dragging along the bottom, but unlike sharp tools and weapons used to take life, these injuries are single, superficial, localized in various areas of the body, including those inaccessible to one's own hand.
Corpses in the water are sometimes damaged by water rats, snakes, crayfish, fish, snails, stingrays, crabs, amphipods, birds, and leeches. Leeches inflict typical damage, forming multiple T-shaped superficial wounds. Fish that gnaw on a corpse leave funnel-shaped depressions on the skin. Crayfish and crustaceans can eat everything soft tissues, penetrate into the cavity and eat out all the internal organs.
Atonal damage occurs in the final periods of drowning during convulsions. They are manifested by abrasions, broken nails, bruises on the forearms, abrasions on the anterolateral surfaces of the body, etc.
Attempts to provide assistance are accompanied by extensive abrasions on the lateral surfaces of the chest. Their presence indicates artificial respiration and chest compressions.
Damage from rough extraction from the water by hooks, "cats", etc. are localized in any areas of the body and reflect the features of their active part.
Inspection of the scene of a drowning accident
The protocol of the inspection of the scene by the investigator must necessarily reflect the temperature of the water and air, the mobility of the water, the speed of the current, the depth of the reservoir, the position of the corpse in the water - face up or down, the method of removing the corpse from the water. The corpse is oriented in relation to the flow of the river, its turn or some other fixed landmark.
By examining the corpse, the presence or absence of objects holding the body on the surface of the water (life jacket, etc.) or contributing to its immersion (stones tied to the body, etc.)
Damage to clothes and shoes is described according to generally accepted schemes. Examining the skin, note their pallor or pinkish color, the presence or absence of "goosebumps" skin.
Cadaveric phenomena are studied with particular care at the scene of the incident, which, after removing the corpse from the water in the air, develop extremely quickly. Inspection focuses on the color of cadaveric spots that have a pinkish tint, indicating the presence of the corpse in the water, their localization on the face and head, indicating the position of the corpse in the water, the degree of development of putrefactive changes, indicating where they are most pronounced, the presence or absence of hair, the degree of their retention by pulling the hair in different areas of the head. In the absence of hair, the area and severity of their holes are indicated.
Examining the face, note the presence or absence of pinpoint hemorrhages in the connective membranes of the eyes, the expansion of their vessels, accumulations of fine bubble foam in the openings of the nose and mouth, the amount and color (white, gray-red), vomit, damage to the protruding areas of the face.
Describing the body of a corpse, they focus on the wrinkling of the areola, nipples, scrotum and penis.
Fixing signs of skin maceration, indicate: localization of areas (palmar surface, nail phalanges, plantar and dorsal surfaces of the feet, etc.), severity of maceration - whitening, loosening, swelling of the epidermis, folding (small or deep), color, degree of retention of the epidermis by sipping , the absence of the epidermis on the limbs, swelling and separation of it in other areas of the body from the underlying layers of the skin.
When examining the hands, the fingers are clenched into a fist, the presence of sand or silt in it, abrasions with traces of sliding on the back surface of the hands, the content of sand, silt under the fingernails, etc.
It is impractical to untie the tied hands and feet at the scene of the incident, since it is better to carefully examine the knots and loops during the examination of the corpse in the sectional room. At the scene, describe the material from which knots and loops are made, their location on the limbs. The load tied to the corpse is not removed at the scene of the incident, indicating only the place of fixation, and sent for examination along with the corpse.
Algae and fungi are described with indication of location, color, degree of distribution over surfaces and areas of the body, type, length, thickness, consistency, strength of connection with the skin.
Before taking a water sample, it is necessary to rinse the liter dishes twice with water from the given reservoir in which the drowning occurred. Water is taken from the surface layer at a depth of 10-15 cm at the place of drowning or the place where a corpse was found. The dishes are closed, sealed by the investigator, the label indicates the date, time and place of taking the sample, the name of the investigator who took the water, and the case number for which the water was taken.
When corpses are found in puddles, containers (including bathtubs), their dimensions, the depth of the container, how and how filled they are, and the temperature of the liquid are noted. If there is no water in the bath, then this must be reflected in the protocol.
Describing the posture of the corpse, they indicate which areas of the body are immersed in the liquid, which are above it, if the body is completely immersed in water, then at what depth and in what layer of water. If the corpse is in contact with the details of the containers, then the contact area of the body and details are described. The diagnosis of drowning is based on a combination of morphological features of the results of laboratory tests and the circumstances of the case, which can be decisive in establishing the type of drowning and death in the water. Drowning - an accident is evidenced by the testimony of eyewitnesses about the circumstances of immersion in water, the use of alcohol (confirmed by the results of laboratory tests), the presence of diseases.
In favor of suicide is the failure to take measures to save, tying a load, tying limbs, the presence of non-fatal injuries that suicides inflict near the water. In these cases, death occurs not from injuries, but from drowning. Criminal deprivation of life is indicated by the presence of injuries that the victim himself could not inflict.
Information necessary for the expert to conduct the examination drowning
In the installation part of the decision, the investigator must reflect: from which body of water the corpse was taken, the place of its discovery - in the water or on the shore, full or partial immersion in water, whether the person was in the water, the temperature of the water and air, the speed of the current, the mobility of the water, the depth of the reservoir , method of extraction from the water (hooks, cats, etc.), testimony of witnesses about the circumstances of the victim’s immersion in water, about trying to stay on the surface of the water, alternating diving with appearing above the surface of the water, information about the previous fight, drinking alcohol, diving, participation in competitions on the water, shipwreck, first aid by a specialist or an outsider, diseases that the victim has at the time of drowning and suffered by him earlier.
The type of drowning (true or asphyxic) determines one or another morphological picture revealed by the study of the corpse.
The external examination of the corpse in the sectional room differs from that at the scene of the incident by the special thoroughness of the study and fixation of the identified features of knots and loops, the weighing of the load used to hold the corpse at the bottom, sketching and detailed photographing of the damage.
In internal research, a variety of sectional techniques are used and additional methods research aimed at detecting damage, changes typical of drowning, and painful changes that contribute to death in the water.
In the soft integument of the head, hemorrhages are found, which may be the result of pulling the victim by the hair. It is obligatory to open the cavities of the middle ear, the sinus of the main bone, with a description of their contents, its nature and quantity, the condition of the eardrums, the presence or absence of holes in them, the study of the muscles of the body, the opening of the spine, the study of the spinal cord, especially in cervical region. Examining the neck and its organs, focus on the presence of soft tissue bundles with blood, fine bubble foam in the airways, its color, quantity, foreign liquid, sand, silt, pebbles (indicating their sizes), note the presence, nature and amount of free fluid in pleural and abdominal cavities. Carefully examining the lungs, fix their size, traces of pressure from the ribs, describe their surface, shape and contours of hemorrhages, pay attention to gas bubbles under the pulmonary pleura, the consistency of the lungs, the color on the cut, the presence and amount of edematous fluid or dryness of the cut surface, reflect the blood filling of the lungs , heart and other organs, the state of the blood (liquid or with bundles). To clarify the dilution of blood with water, a simple test is used, which is made by applying a drop of blood from the left ventricle to filter paper. Diluted blood forms a lighter ring, proving hemolysis and blood thinning.
In the study of the gastrointestinal tract, the presence of foreign bodies and fluid in the stomach and duodenum, its nature and amount (free fluid, liquefaction of the contents) are noted. The stomach and duodenum are tied up before being removed from the corpse, and then, above and below the ligatures, they are cut and placed in a glass vessel to settling the liquid. Dense particles will settle to the bottom, a layer of liquid above them sometimes covered with foam. The presence of fluid in the duodenum is one of the most reliable signs of drowning, indicating increased peristalsis, but this sign is of diagnostic value only on fresh corpses. Particular attention is paid to the small curvature of the stomach, where there may be ruptures of the mucous membrane. The diagnosis of drowning is confirmed by laboratory tests for the presence of elements of diatom plankton in the internal organs. For research, an unopened kidney is taken with a ligature applied to the leg in the gate area, about 150 g of the liver, the wall of the left ventricle of the heart, brain, lung, fluid from the middle ear cavity or sinus of the main bone. In putrefactive corpses, the femoral or humerus. In addition to research on diatom plankton, it is necessary to produce and histological examination in order to determine the changes due to drowning and diseases that contribute to death in the water.



