Classification of hemolytic disease of the newborn. Exchange transfusion Forms of HDN and their clinical features
Hemolytic disease of the newborn (HDN)- a disease caused by the incompatibility of the blood of the mother and the fetus for various antigens that are present in the blood of the latter (inherited from the father) and absent in the blood of the mother. Most often, the disease develops when the blood of the mother and fetus is incompatible with the Rh antigen (1 case per 200-250 births). It should be noted that there are several types of Rh antigen, designated according to Wiener - Rh 0, Rh ", Rh". At the suggestion of Fisher-Reiss, the types of the Rh antigen began to be designated respectively by the letters D, E and C. Usually, the Rh conflict develops with incompatibility for Rh 0, i.e. (D) antigen, for other types - less often. Cause hemolytic disease there may be incompatibility for antigens of the ABO system.
Hemolytic disease of the newborn is possible when there is a mismatch between the blood of the mother and the fetus and other antigens: M, N, S, P or systems Lutheran (Lu), Levi (L), Kell (Kell), Dufy (Fy), etc.
Pathogenesis. If the blood of the mother and fetus does not match, antibodies are produced in the body of a pregnant woman, which then penetrate during pregnancy through the placental barrier into the blood of the fetus and cause destruction (hemolysis) of its red blood cells. As a result of increased hemolysis, a violation of bilirubin metabolism occurs. Violation of the latter contributes to liver failure in the form of immaturity of the glucuronyltransferase enzyme system. The latter is responsible for the conjugation of indirect bilirubin with glucuronic acid and its transformation into non-toxic direct bilirubin (bilirubin-glucuronide).
The following options for the penetration of antibodies through the placenta are possible:
- during pregnancy, which leads to congenital forms of HDN (the birth of macerated fetuses, edematous, anemic, icteric forms);
- during childbirth, which leads to the development of postpartum icteric form;
Anti-Rh antibodies are formed in 3-5% of women with Rh-negative blood during pregnancy with a fetus with Rh-positive blood. Usually children with Rh conflict are born with HDN from the 2nd-3rd pregnancy, less often from the 1st pregnancy in cases of sensitization in the past by blood transfusions without taking into account the Rh factor. In some women, antibodies may be low and antibodies do not cross the placenta, and an Rh-sensitized woman may have a healthy Rh-positive baby after giving birth to children with HDN. With ABO incompatibility, the disease develops already during the 1st pregnancy.
The severity of HDN is not the same, it depends on the amount of antibodies that have penetrated from the mother to the fetus, the compensatory capabilities of the fetal body. Hemolytic disease of the newborn manifests itself in 3 main forms: anemic, icteric, edematous.
Clinic. Hemolytic disease of the newborn can manifest itself in the following ways:
- the child dies during fetal development (on the 20-30th week);
- born with universal edema;
- in the form of early onset severe jaundice or
- severe anemia.
Common symptoms for all forms of the disease are normochromic anemia of a hyperregenerative nature with the presence in the blood of young forms of erythrocytes (erythroblasts, normoblasts, an increased number of reticulocytes), enlargement of the liver and spleen.
edematous form the disease develops with prolonged action of isoantibodies during pregnancy; the fetus does not die, since toxic products are excreted through the placenta into the mother's body. Due to the adaptive reactions of the fetus, foci of extramedullary hematopoiesis are formed, the spleen (5-12 times), liver, heart, endocrine glands increase. Liver functions are disturbed, especially protein-forming, vascular permeability increases, hypoalbuminemia develops. All this leads to pronounced edema of the subcutaneous fat layer, accumulation of fluid in the cavities (pleural, abdominal) and an increase in fetal weight by almost 2 times against the age norm. Anemia (Hb 35-50 g/l, erythrocytes 1-1.5 x 10 12 /l), erythroblastemia are pronounced. The placenta is sharply enlarged, edematous. Metabolic disorders in some cases can cause fetal death before birth or during childbirth. The edematous form is characterized by an extremely severe course and in most cases ends in death. A child born alive dies within minutes or hours.
Currently, some children with generalized congenital edema can be saved by the careful use of exchange transfusions.
icteric form develops under the influence of isoantibodies on a sufficiently mature fetus. The baby is usually born at term, with a normal body weight, with no visible changes in skin color. HDN develops a few hours after birth. Already on the 1st-2nd day of his life, jaundice is detected, which is rapidly increasing; less often a child is born with icteric coloration of the skin. Amniotic fluid and primordial lubrication have the same color. All children with the icteric form of the disease have an increase in the liver, spleen, lymph nodes, and sometimes the heart; an increase in the content of bilirubin in the umbilical cord blood - above 51 µmol / l (in healthy newborns it ranges from 10.2-51 µmol / l, averaging 28.05 µmol / l according to Van den Berg). In the next 72 hours in children with HDN, the level of bilirubin increases rapidly, the hourly increase is from 0.85 to 3.4 µmol/l.
You can determine the hourly increase in bilirubin using the formula:
where B t is the hourly increase in bilirubin; In n 1 - the level of bilirubin at the first determination; In n 2 - the level of bilirubin in the second determination; n 1 - the age of the child in hours at the first determination; n 2 - the age of the child in hours at the second determination of bilirubin.
The immaturity of the enzyme systems of the liver of a newborn leads to the accumulation of indirect bilirubin in the blood. Indirect bilirubin is a cytoplasmic poison and causes damage to hepatocytes (liver cells), myocardial muscle cells, but especially neurons ( nerve cells).
An intensive increase in the content of indirect bilirubin (an hourly increase from 0.85 to 3.4 μmol / l), if measures are not taken to reduce it, quite soon (after 24-48 hours) leads to its excessive accumulation and the appearance of pronounced jaundice in the child with symptoms of bilirubin intoxication and damage to the central nervous system(nuclear jaundice, or bilirubin encephalopathy), which is accompanied by a deterioration in the child's condition: lethargy appears, the child sucks worse, frequent regurgitation, vomiting appear, tonic convulsions are often noted (on the 4-5th day of life), stiff neck, oculomotor disorders and spasms of the gaze (a symptom of the "setting sun" - an involuntary downward turn of the eyeballs, in connection with which a strip of sclera is visible between the upper edge of the cornea and the upper eyelid); breathing becomes slow and irregular, bouts of cyanosis develop, congenital reflexes of Moreau, Robinson, Babkin decrease. In addition, there is a deposition of crystalline bilirubin in the medulla of the kidneys - a bilirubin infarction of the kidneys develops. Impaired liver function in HDN is manifested not only by a violation of the formation of direct bilirubin, but also by a decrease in the synthesis of prothrombin and protein. The level of prothrombin in the blood decreases. Bleeding time is increased. Loading the liver with hemolysis products often leads to a violation of the excretion phase with the development of obstructive jaundice - the so-called bile thickening syndrome. In this syndrome, the feces are discolored (usually in children with this form of feces are bright yellow), the liver is even more enlarged, the level of direct bilirubin in the blood rises, there are a lot of bile pigments in the urine (Gmelin's reaction is positive).
The toxic properties of indirect bilirubin begin to appear when it is not bound to plasma albumin (the bilirubin-binding ability of blood plasma is reduced) and therefore easily penetrates beyond the vascular bed. With a sufficient amount of albumin in the blood, brain damage begins to develop at a bilirubin level that is significantly higher than the critical one.
The danger of damage to the central nervous system in the form of bilirubin intoxication (nuclear jaundice) appears with an increase in the level of indirect bilirubin in a full-term baby above 306-340, in a premature baby - from 170 to 204 µmol / l. The resulting bilirubin encephalopathy can be fatal as early as 36 hours after the birth of a child. Children who remain alive are significantly behind in mental development.
In the future, there is a moderate delay in the overall development of the child. Due to the suppression of immune defense mechanisms, such children easily develop pneumonia, omphalitis, and sepsis. Bilirubin intoxication, complications of infectious diseases, anemia, changes in the internal organs cause a severe course of congenital icteric form of HDN with a large number of deaths. Timely treatment patients can prevent adverse outcomes of this form of HDN.
anemic form proceeds relatively easily. It develops as a result of a short exposure of a small dose of maternal isoantibodies to the fetus; at the same time, the damage to the fetus is small, the products of hemolysis are discharged by the placenta into the mother's body. After birth and cessation of placental function, with sufficient liver function, there is no jaundice, the child develops normally in the presence of anemia. These cases are rare. The main symptom of this form of the disease is pallor. skin in combination with a low amount of hemoglobin and red blood cells, an increase in immature forms of red blood cells (erythroblasts, normoblasts, reticulocytes). The liver and spleen are enlarged. Anemia develops at the end of the 1st - beginning of the 2nd week of life, the content of hemoglobin and erythrocytes decreases, anisocytosis, polychromasia, erythroblastosis appear. The liver and spleen are enlarged.
Usually, the pallor of the skin is clearly detected from the first days of life, but in milder cases it is masked by physiological erythema and transient jaundice and is clearly detected only by the 7-10th day of life. With fractional transfusions of Rh-negative blood, the child recovers quickly.
The development of hemolytic disease of the newborn is not always determined by the height of the titer of isoimmune antibodies in pregnant women. The degree of maturity of the body of the newborn matters - a more severe course of the disease is noted in premature babies.
Hemolytic disease of the newborn, associated with the incompatibility of the blood of the mother and child according to the antigens of the ABO system, occurs with the same frequency as HDN, due to Rh incompatibility. HDN associated with group incompatibility occurs when the mother has 0 (I) blood type, and the child is A (II) or B (III). Usually the disease occurs during the 1st pregnancy. Clinically, hemolytic disease of the newborn associated with ABO incompatibility proceeds in a mild form (in 90% of cases), resembling transient jaundice along the way. However, with a frequency of one case per 2000-2200 births, the disease can proceed in the form of severe jaundice and be complicated by bilirubin encephalopathy if active measures are not taken in a timely manner to reduce the level of bilirubin, including exchange transfusion.
The cause of the severe course of the process in such cases is concomitant acute and chronic diseases of the mother during pregnancy, causing an increase in the permeability of the placental barrier for isoantibodies. HDN associated with group incompatibility is not observed in the form of edema.
Early diagnosis. Allocate pregnancy, "threatened" by the development of hemolytic disease in the fetus. The assumption about the possibility of developing HDN should arise when examining a pregnant woman in a antenatal clinic. Rh-negative blood in the mother and Rh-positive in the father, indications in the anamnesis of the mother for blood transfusion without taking into account the Rh factor should raise the possibility of HDN in the unborn child. The presence of a aggravated anamnesis (stillbirth, spontaneous miscarriages, the birth of infants with HDN, a lag in the mental development of children from previous pregnancies) makes us think about the possibility of a severe course of HDN in the expected child and taking such a woman into special account with the need to conduct a complex of special studies. First of all, the blood of a woman with a Rh-negative affiliation should be examined for the presence of Rh antibodies: if the latter are detected, preventive actions aimed at weakening the phenomena of isoimmunization.
The diagnosis of a disease in an intrauterine fetus can be established on the basis of the results of a study of amniotic fluid obtained using amniocentesis (their optical density, their bilirubin content).
It is important to establish a diagnosis of HDN with an assessment of the severity of the disease immediately after the birth of the child. The criteria for the presence of the disease are: Rh-negative blood of the mother and Rh-positive blood in a newborn with the presence of Rh antibodies in the blood of the mother; with group incompatibility - the presence of group 0 (I) in the mother and A (II) or B (III) - in the child with the determination in the mother's blood serum of a high titer of isoimmune α- or β-agglutinins in the protein medium.
Table 1. Differential diagnostic symptoms in Rh- and AB0-incompatibility
| Incompatibility | Manifestations | ||||||||
| Clinical | paraclinical | ||||||||
| General state | Jaundice | Anemia | Liver, spleen | Coombs reaction | Munch Andersen reaction | Erythroblasts, reticulocytes | Morphology of erythrocytes | ||
| appearance | intensity | ||||||||
| Rh | disturbed | up to 14 h | + + + | + - + + | increased | + | (-) | + + | macrocytes |
| AB0 | good | 1-2 days | + - + + | - | not enlarged | (-) | (+) | + | spherocytes |
As a rule, in the case of an extremely severe course of HDN, the diagnosis does not cause difficulties even in the absence of anamnestic data; amniotic fluid and labor lubrication are yellow or green, the child is edematous, icteric or pale, the liver and spleen are significantly enlarged.
In cases where the condition is unclear, early diagnosis and prognosis of the disease is important clinical analysis blood of a newborn, especially the umbilical cord, since changes in it with HDN are detected much earlier than other clinical signs of the disease.
The following indicators of umbilical cord blood indicate the presence of HDN:
- hemoglobin below 166 g/l;
- the presence of erythroblasts and normoblasts in an amount of more than 10 per 100 leukocytes;
- positive Coombs test with Rh-conflict; with a conflict in the ABO system, the Coombs test is negative;
- the content of bilirubin is above 51 μmol / l according to Van den Berg;
- a decrease in the level of blood protein to 40-50 g / l.
If cord blood was not taken for research, then if there is a suspicion of the presence of hemolytic disease due to the early onset of jaundice (on the first day after birth), it is necessary to assess the severity of hemolytic disease according to the hourly increase in bilirubin.
It is difficult to make an early diagnosis in cases where TTH is caused by other antigens. To do this, a study of the mother's blood serum for the presence of antibodies to rare antigens is carried out. While the cause of the disease is being clarified, treatment should be aimed at combating intoxication with indirect bilirubin.
Differential Diagnosis. In the differential diagnostic relation, one should mainly bear in mind hyperbilirubinemia with an increase in indirect bilirubin and hyperbilirubinemia, in which there is hemolysis, i.e., which occur with erythroblastosis and reticulosis in the peripheral blood:
- due to congenital or acquired defects of the erythrocyte membrane with typical changes in their morphology, such as spherocytosis, elliptocytosis, stomatocytosis and pycnocytosis;
- as a result of enzymatic defects in erythrocytes - glucose-6-phosphate dehydrogenase (the most common enzymatic-metabolic disease), pyruvate kinase, etc.
The main differential diagnostic criteria are positive Coombs or Munch-Andersen tests for hemolytic disease of the newborn and proof of enzyme deficiency. These include thalassemia and disseminated intravascular coagulopathy. To confirm the diagnosis of alpha thalassemia, the family history of the child is important and, mainly, the establishment of Barth's hemoglobin by means of hemoglobin electrophoresis. The diagnosis of disseminated intravascular coagulopathy is facilitated by characteristic changes in blood coagulation factors or global tests, such as prothrombin time, thrombin, heparin time, platelet count, fragmented erythrocytes.
Less well known and more difficult to diagnose are metabolic endocrine hyperbilirubinemias. Crigler-Najjar syndrome (familial non-hemolytic hyperbilirubinemia with kernicterus) is characterized by indirect hyperbilirubinemia without evidence of hemolysis and is transmitted as an autosomal recessive disease. Parents have a reduced ability to conjugate bilirubin without jaundice. Jaundice in a child appears already in the first days after birth, sometimes with very high values of bilirubin. In this regard, there may be a need for an exchange transfusion of blood.
Transient familial neonatal hyperbilirubinemia or Lucey-Driscoll syndrome manifests as an increase in indirect bilirubin without evidence of hemolysis. It is believed that it occurs under the influence of the inhibitory effect of some factor, in all likelihood, a steroid in pregnant women, which disrupts the normal conjugation of bilirubin. With severe jaundice in some children, an exchange transfusion of blood is necessary.
Jaundice regularly accompanies neonatal hypothyroidism with its characteristic appearance, hypotension, rough voice, large abdomen, and generally delayed development of the bone nuclei and specific abnormalities in the level of thyroid hormones. In children, indirect hyperbilirubinemia is seen in newborns with hypopituitarism or anencephaly. Pronounced jaundice in these two groups of diseases is associated with the presence of hypothyroidism.
Many medicines, hormones and other substances and conditions play a role in the appearance of hyperbilirubinemia in newborns, such as sulfonamides, vitamin K, especially in high doses, novobiocin, hypoxia, acidosis, etc. Three α-20-β-pregnadiol and the milk of some mothers are also the cause of this painful condition.
In newborns whose mothers are sick diabetes, hyperbilirubinemia with an increase in indirect bilirubin without hemolysis is observed more often and is more pronounced than in healthy newborns. It appears by the 3rd day after birth, when the hematocrit also rises, which currently explains the hyperbilirubinemia in these children.
Jaundice and anemia can be observed with sepsis, cytomegaly, toxoplasmosis, congenital infectious hepatitis, syphilis and other diseases.
Treatment of HDN- complex, aimed at the fastest removal of toxic products of hemolysis from the body of a newborn, mainly indirect bilirubin, as well as antibodies that contribute to the continuation of the hemolytic process, and to increase the functional capacity of various systems and organs, especially the liver and kidneys.
The most effective method of combating hyperbilirubinemia in severe and moderate forms of the disease is early exchange blood transfusion at the rate of 150-180 ml/kg of newborn weight. In case of a Rh-conflict, one-group Rh-negative blood is transfused, in case of an ABO-conflict, erythrocytes of the 0 (I) group, suspended in the plasma of the AB (IV) group, are transfused. For exchange transfusion, the donor's blood (stabilizers 7, 5) must be fresh, no more than 3 days of storage after collection.
The indication for exchange transfusion is:
- an increase in the content of bilirubin in the blood plasma on the first day to 171.04 µmol/l
- an increase in bilirubin in the blood by 0.85 µmol / l per hour
Early applied exchange transfusion allows correcting anemia, removing a significant part of sensitized erythrocytes, which, in turn, limits the development of the hemolytic process and eliminates a certain amount of bilirubin before it is distributed in larger quantities in the extravascular space. In the presence of severe anemia (hematocrit 35% or less), an exchange transfusion is used - 25-80 mg / kg body weight of erythrocyte mass 30 minutes after birth in order to increase the hematocrit to 40%. The possibility of hypovolemia in such children is indicated. Therefore, it is recommended that before proceeding with manipulations in order to change blood volume, a thorough measurement of venous and arterial pressure should be carried out.
The most expedient and technically easy to perform is an exchange transfusion through the umbilical vein (the first 3-5 days of life). First, 10 ml of blood is released through the catheter inserted into the umbilical vein, then the same amount of donor blood is injected, the duration of the procedure is 1 ½ - 2 hours (the speed of the blood replacement operation is 2-3 ml / min), at the end of the transfusion, it is injected for 50 ml of blood is more than is excreted. After replacing every 100 ml of blood, the child must be injected intravenously with 1 ml of a 10% solution of calcium chloride. After blood transfusion, detoxification therapy is carried out: abundant fluid intake, intravenous transfusion of plasma, albumin, glucose (100-250 ml).
Due to the fact that the citric acid of banked blood for exchange transfusion is very quickly metabolized in the liver to bicarbonates, most children have no difficulty during the transfusion itself without alkalinization, if it is done very slowly. However, after transfusion, some newborns develop alkalosis, which can last for 72 hours. It is dangerous to infuse acid-preserved blood, as this can directly affect the myocardium and cause cardiac arrest. In this regard, in children in a state of shock or significant metabolic acidosis, it is recommended to use alkalized blood. On the other hand, it should not be forgotten that with the introduction of alkalizing agents there is a danger of an increase in osmolarity with its consequences. Elimination of 60 ml of plasma from a donor's blood prior to exchange transfusion reduces acidity and citrate load and normalizes hematocrit.
Some authors recommend using heparinized blood for exchange transfusion. It should be noted that the content of ionized calcium, electrolytes, acid-base balance and blood sugar levels do not change. But as a consequence, the use of heparin significantly increases the level of non-esterified fatty acids, which can replace bilirubin in the albumin-bilirubin complex. It should also be borne in mind the possible changes in the coagulation parameters of the newborn. The most important disadvantage of heparinized blood when used for exchange transfusion is that it should be used no later than 24 hours from the moment it is taken from the donor and preserved.
It follows from the foregoing that exchange transfusion of blood in newborns is associated with a number of complications, if we do not take into account the biochemical changes that may occur during this manipulation.
Phenobarbital is used to improve liver function. Treatment with phenobarbital is due to its inducing effect on the activity of glucuronyl transferase and the established increased ability of ligandin to bind bilirubin in the hepatocyte. It is used from the first or second day at a dose of 5 mg/kg of body weight 2-3 times a day, some clinicians recommend up to 10 mg/kg of body weight per day. Consider that this treatment cannot give result at already shown jaundice.
In case of violation of the bilirubin excretory function of the liver and the development of "bile thickening syndrome", a 5-10% solution of magnesium sulfate 5 ml 2-3 times a day, 10-20% solution of xylitol, holosas, sorbitol can be administered orally. Duodenal sounding for the purpose of bile drainage is also effective. However, treatment with agar, activated charcoal and magnesium sulfate to reduce enterohepatic circulation and resorption of bilirubin is rejected by most authors on the basis of daily practice, since it does not give positive results.
The child is prescribed: feeding with donor milk, breastfeeding not earlier than the 10th-12th (according to indications and later) days of life, adenosytrophosphoric acid (ATP) 0.5 ml intramuscularly, methionine, ascorbic acid, pyridoxine, cyanocobalamin, tocopherol 10 each mg by mouth. Inside, prednisolone is also prescribed at 1-1.5 mg / kg for 7-8 days.
Phototherapy is also shown (irradiation of newborns with lamps of "blue or blue" light): sessions of 3 hours at intervals of 1-2 hours, i.e. up to 12-16 hours a day (phototherapy takes from 2 to 6 days). Under the action of light, bilirubin is oxidized, turning into biliverdin and other non-toxic substances.
Currently, phototherapy is the most appropriate method for regulating bilirubin levels in newborns. Statistics show that after the introduction of phototherapy into practice, the number of exchange transfusions has decreased significantly. The method is based on the photoisomerization of bilirubin-IX-α and the production of photobilirubin, which is very quickly excreted in the bile. This process takes place in the skin and its capillary network at a depth of 2 mm. The indications for this treatment are mainly hyperbilirubinemia of prematurity with Rh- and ABO-incompatibility, usually after exchange transfusion. There are reports of a more favorable effect of phototherapy than exchange transfusion in a newborn with non-hemolytic hyperbilirubinemia. The indications for turning on phototherapy are shown in Table 1. 2, in which each individual case is scored according to postnatal age, birth weight, birth pathology, and bilirubin level.
In the presence of perinatal hypoxia, respiratory distress, metabolic acidosis (pH 7.25 or below), hypothermia (below 35°C), low serum protein (50 g/l and below), cerebral impairment, birth weight less than 1500 g, and symptoms clinical deterioration, phototherapy and exchange transfusion should be used, as in the subsequent, higher bilirubin group indicated in Table 2.
Table 2. The main directions in the treatment of hyperbilirubinemia (according to Brown et al.)
| Whey bilirubin (µmol/l) |
Body mass at birth |
< 24 ч | 24-48 hours | 49-72 h | > 72 |
| 85,52 | All | Under control | |||
| 85,52 - 153,93 | All | Phototherapy for hemolysis | Under control | ||
| 171,04 - 239,45 | < 2500 г | Exchange transfusion with hemolysis | Phototherapy | ||
| > 2500 g | Study at a bilirubin level of 12 mg | ||||
| 256,56 - 324,9 | < 2500 г | Exchange transfusion | Sometimes exchange transfusion | ||
| > 2500 g | Phototherapy | ||||
| 342,08 | All | Exchange transfusion | |||
However, with longer use, phototherapy leads to a number of side effects: retinal damage, deviations of embryogenesis (experiments on animals), thrombocytopenia, pallor of the skin and the "copper child" syndrome, observed with data indicating holostasis. It is hypothesized that the retention of some phototherapy product is the cause of this particular skin color in the child. As side effects, the presence of green feces and the loss of fluids and some salts with feces are also described.
In practice, the following precautions should be taken into account:
- Before using phototherapy, the etiology of hyperbilirubinemia should be determined, if possible, in order to avoid missing a life-threatening condition.
- Protect eyes and gonads
- Monitor baby's temperature
- Control the water balance (twice a day, measure the child's temperature, amount and specific gravity of urine, hematocrit) and, if necessary, introduce more liquid
- Examine bilirubin every 12 hours, and more often if indicated, without relying on an assessment of the severity of jaundice by skin color
- Control platelet count
- Examine hematocrit, especially in hemolytic disease
- Use a lactose-free nutrient mixture for dyspeptic feces containing an increased amount of reducing substances
The issue of repeated replacement blood transfusions is decided by the rate of increase in the level of bilirubin in dynamics. In full-term newborns, such indications occur with an hourly increase in bilirubin content of more than 5.13 μmol / l, or one should focus on the level of bilirubin, which exceeds critical numbers (according to the Polachek scale): the level of indirect bilirubin in full-term infants is over 306 and in premature infants - over 204 μmol / l.
With the development of anemia in a child (decrease in hemoglobin below 80 g / l), anti-anemic treatment is carried out by fractional blood transfusions of 20-25 ml 2-3 times. Children with HDN need careful care, proper feeding.
If the child has not received an exchange transfusion, then it is necessary to feed him with donor milk for the first 2-3 weeks, focusing not only on the content of Rh antibodies in the mother's milk, but also on the severity of the disease.
Babies treated with exchange transfusions can start breastfeeding as soon as early dates(from the 5-7th day of life).
After treatment in the acute period of the disease, upon discharge from the maternity hospital or hospital, the child needs to do a blood test every 10-14 days from 3 weeks of age to 2 months and, if hemoglobin decreases, take a course of treatment with vitamin B 12, 50 mcg every other day, 10 -12 injections per course. Children with damage to the central nervous system are prescribed a course of vitamin B 12 - 50 mcg every other day, for a course of 20 injections.
Forecast. Children who have had hemolytic disease of the newborn and are promptly treated with sufficient volume of exchange transfusions usually develop well in the future. In mild and moderate forms of jaundice, the prognosis is favorable. Patients with HDN in the form of severe jaundice with hyperbilirubinemia above the "critical" numbers in the acute period, not treated in a timely manner by exchange transfusions, may die during the first days of life. In the survivors, during the development in the acute period of nuclear jaundice, an organic lesion of the central nervous system is later detected, which is manifested by a lag in physical and mental development, hearing loss and speech impairment.
Children with residual effects in the state of the central nervous system need restorative therapy. They should be well cared for, massaged, prescribed drug therapy- glutamic acid, vitamins of the B complex (B 6, B 1, B 12), aminalon.
Preventive actions to prevent HDN or reduce its severity should be carried out already in the antenatal clinic and are as follows:
- Determination of the Rh factor and blood type in all pregnant women
- All women with Rh-negative blood and with the 0 (I) group must be registered, a detailed anamnesis should be collected from them, and it should be found out if they have had a blood transfusion in the past without taking into account the Rh factor. In all these women, it is necessary to determine the titer of Rh antibodies regularly (once a month). With an unfavorable (according to HDN) history, a high titer of antibodies, an early (2 weeks) delivery is performed.
- At present, desensitization with Rh-negative blood is successfully carried out through a number of special measures: in the last 3 months of pregnancy, this is the grafting of a skin flap from the husband, the introduction of a primigravida (if the child has Rh-positive blood) immediately after birth (during the first 72 hours after birth) anti-Rh-gamma-immunoglobulin (200-250 mcg), prepared from the blood of Rh-negative women who gave birth to a Rh-positive child. In this way, the goal is to neutralize the Rh factor as an antigen.
- Pregnant women with Rh-negative blood, who have a rapidly increasing antibody titer, especially if previous pregnancies ended unsuccessfully, should be placed in a specialized maternity hospital to control the course of pregnancy. In pregnant women with a high titer of antibodies who are in the hospital, it is necessary to monitor the dynamics of the level of bilirubin in the fetus. With high titers of bilirubin, an earlier delivery may be necessary if the optimal degree of fetal maturity (which is possible with modern studies) is ascertained, allowing it to cope with extrauterine life. Cases of intrauterine exchange transfusion of blood in the fetus are described.
- With Rh-negative blood, it is necessary to maintain the first pregnancy, since usually the first child is born normal, the threat of HDN in the children of such women increases with repeated pregnancies.
HDN due to immunological conflict with incompatibility of the blood of the fetus and mother for erythrocyte antigens is the most common cause pathological neonatal jaundice. In this regard, any newborn with pathological jaundice must first of all exclude or confirm the presence of HDN.
Etiology. There are 14 main erythrocyte group systems that combine more than 100 antigens. HDN usually causes incompatibility between the fetus and mother for Rh or ABO antigens.
It has been established that the Rh-antigenic system contains the main antigens, designated either C, c; D, d; E, e (Fischer's terminology), or Rh", hr", etc. (Winner's terminology).
Rh-positive erythrocytes contain the D-factor (Rho-factor, in Winner's terminology), while Rh-negative erythrocytes do not have it. D-antigen is a lipoprotein located on the inner surface of the plasma membrane of erythrocytes, and when they write d-antigen, they mean the absence of D-antigen. Rh-positive individuals can be homozygous (DD) - 44% or heterozygous (Dd) - 56%, i.e. 25% of children from Rh-negative mothers and Rh-positive fathers will be Rh-negative.
Sensitization of an Rh-negative mother to the Rh-D antigen usually leads to Rh-THN, which usually precedes pregnancy.
Sensitizing factors are primarily previous pregnancies (including ectopic and ended in abortion), and therefore Rh-HDN, as a rule, develops in children born not from the first pregnancy.
AV antigens are located on the outer surface of the plasma membrane of red blood cells. ABO-incompatibility of the fetus and mother is noted in 1-3% of cases of incompatibility between the fetus and mother. Incompatibility for AB0 antigens leading to TTH usually occurs with maternal blood type 0 (I) and child blood type A (II).
If HDN develops with a double incompatibility of the child and mother, i.e. mother 0 (I) Rh-negative, and the child is A (II) Rh-positive or B (III) Rh-positive, then, as a rule, it is due to A- or B-antigens.
ABO-THN can occur already during the first pregnancy, in violation of the barrier functions of the placenta due to the presence of somatic pathology in the mother, preeclampsia, which led to intrauterine fetal hypoxia. Sensitization to AV antigens can occur without blood transfusions and pregnancies, and in everyday life - with food, with certain infections, preventive vaccinations (for example, diphtheria toxoid).
Pathogenesis. Fetal erythrocytes are regularly detected in the mother's bloodstream from 16 to 18 weeks of gestation. During the first pregnancy, fetal erythrocytes (even in the amount of 0.1 ml) that have entered the mother's bloodstream and have a D-antigen (absent in the mother) start the synthesis of Rh antibodies related to Ig M (which do not penetrate the placenta), and then - antibodies of the Ig G class, which can already cross the placenta.
During pregnancy, the mother's primary immune response is reduced. After the birth of a child and due to the appearance of a large number of erythrocytes of the child in the mother's bloodstream, which penetrated there during childbirth, and due to the removal of immunosuppression, an active synthesis of Rh antibodies occurs. Therefore, the introduction of exogenous Rh antibodies (anti-D-immunoglobulin) within 24-72 hours after childbirth or abortion (D-antigens appear in the embryo at the beginning of the second month of gestational age) is an effective method for reducing Rh sensitization and the frequency of Rh-THN by 95%.
In the early stages of HDN, anemia is macrocytic and hyperregenerative, with high levels of erythropoietin and reticulocytes in the blood, but by the 3rd week of life, anemia becomes normocytic and hyporegenerative with low levels of erythropoietin and reticulocytes.
The inhibition of erythropoiesis occurs especially early in children with HDN who received intrauterine exchange transfusion.
The main damaging factor in HDN is a complication of increased hemolysis - UNCONJUGATED HYPERBILIRUBINAMIA .
Hemolysis of erythrocytes in HDN occurs in macrophages of the liver, spleen, and bone marrow, although in severe forms of the disease, hemolysis can also be intravascular. Incomplete anti-erythrocyte antibodies related to Ig G damage the erythrocyte membrane, leading to an increase in its permeability and metabolic disorders in the erythrocyte. These erythrocytes, changed under the action of antibodies, are actively captured by macrophages of the listed organs and die prematurely.
The resulting large amount of NB entering the blood cannot be excreted by the liver, and hyperbilirubinemia develops.
If hemolysis is not intense, with a small amount of incoming maternal antibodies, the liver actively removes NB, then the child's clinical picture of HDN is dominated by anemia in the absence or minimal severity of jaundice.
If anti-erythrocyte alloimmune antibodies penetrated to the fetus for a long time and actively during pregnancy before the onset of labor, then intrauterine maceration of the fetus or edematous form of HDN develop. The edematous form of HDN is caused by maternal T-killers that penetrated the fetus and caused a graft-versus-host reaction, as well as maternal antibodies to fetal tissues.
In most cases, the placenta prevents the penetration of alloimmune antibodies to the fetus.
At the time of birth, the barrier properties of the placenta are sharply violated, and maternal isoantibodies enter the fetus, which, as a rule, causes the absence of jaundice at birth and its appearance in the first hours and days of life.
Anti-erythrocyte antibodies can be supplied to the baby with mother's milk, which increases the severity of HDN.
In the genesis of hyperbilirubinemia, not only active hemolysis is important, but also a defect in liver function (its conjugation systems), which is typical for all newborns of this age and is more pronounced in HDN.
Unconjugated hyperbilirubinemia leads to damage to various organs and systems (liver, kidneys, lungs, heart), but the main one is damage to the nuclei of the base of the brain. This state, at the suggestion of G. Schmorl (1904), was called " NUCLEAR JAUNDICE ».
The brain of a newborn is characterized by:
The absence of ligandin, a specific protein that binds NB in the cytoplasm;
Very low activity of the bilirubin oxygenase system, which oxidizes NB and makes it non-toxic;
Reduced ability to clear cerebrospinal fluid from bilirubin;
Increased capillary permeability;
Large extracellular space in the brain, especially in preterm infants.
It is believed that the process begins with the introduction of NB into the axons of nerve cells. Newborns with a high level of NB in the blood have clear signs of demyelination nerve fibers, edema, necrosis and death of neurons.
The occurrence of nuclear jaundice depends on the level of NB in the blood. At the level of NB in the blood serum of 428-496 µmol/l, it develops in 30% of full-term children, and at a level of 518-684 µmol/l - in 70%. However, bilirubin encephalopathy can also occur with a much lower level of NB in the blood, for example, in preterm infants with a gestation period of less than 28 weeks - even with hyperbilirubinemia of 171-205 μmol / l.
Risk factors for bilirubin encephalopathy are:
Factors that damage the blood-brain barrier and increase its permeability - hyperosmolarity (including due to hyperglycemia), severe respiratory acidosis, hemorrhages in the brain and its membranes, convulsions, neuroinfections, endotoxinemia, arterial hypertension;
Factors that increase the sensitivity of neurons to the toxic effect of NB are prematurity, severe asphyxia (especially complicated by severe hypercapnia), hypothermia, starvation, severe hypoglycemia and anemia;
Factors that reduce the ability of albumin to bind NB firmly - prematurity, hypoalbuminemia, acidosis, infections, hypoxia or substances competing with NB for binding to albumin, intravascular hemolysis, elevated level in the blood of non-esterified fatty acids, some drugs (sulfonamides, alcohol, furosemide, diphenin, diazepam, indomethacin and salicylates, methicillin, oxacillin, cephalothin, cefoperazone).
If a child has 2-3 of the mentioned factors, an exchange transfusion is done with lower values of hyperbilirubinemia.
The initial stages of bilirubin brain damage are, in principle, reversible.
On the 3rd-5th day of life, there may be a significant rise in bilirubin diglucuronide, i.e. direct bilirubin. This is due to the syndrome of "bile thickening" and impaired liver function.
Classification. HDN is classified:
By type of conflict (Rh-, AB0-, other antigenic systems);
According to the clinical form (intrauterine fetal death with maceration, edematous, icteric, anemic);
According to the severity in icteric and anemic forms (mild, moderate and severe);
By complications (bilirubin encephalopathy - nuclear jaundice, other neurological disorders; hemorrhagic or edematous syndrome, damage to the liver, heart, kidneys, adrenal glands, "bile thickening" syndrome, metabolic disorders - hypoglycemia)
By the presence of concomitant diseases and background conditions (prematurity, intrauterine infections, asphyxia, etc.).
easy current HDN is diagnosed in the presence of moderate clinical and laboratory data or only laboratory data. In this case, in the absence of any complications, severe background conditions and concomitant diseases, only phototherapy is required. The level of hemoglobin in cord blood in the first hours of life is more than 140 g/l, NB in cord blood is less than 68 µmol/l.
O moderate HDN is evidenced by hyperbilirubinemia, requiring exchange transfusion or hemosorption, but not accompanied by bilirubin intoxication of the brain or the development of other complications. Jaundice appears in the first 5 hours of life with Rhesus conflict or in the first 11 hours of life with AB0 conflict, the hemoglobin concentration in the first hour of life is less than 140 g / l and the level of bilirubin in cord blood is more than 68 μmol / l. In the peripheral blood, there are nuclear forms of erythrocytes, leukemoid reaction, thrombocytopenia. There is hepatosplenomegaly. A child with jaundice has three or more risk factors for brain bilirubin toxicity. Early exchange transfusion combined with intensive phototherapy is necessary. In such children, hyporegenerative anemia quite often develops after an acute period, requiring the administration of exogenous erythropoietin.
On the severe course HDN indicates the edematous form of the disease, severe anemia (hemoglobin less than 100 g / l) or jaundice at birth (hyperbilirubinemia more than 85 μmol / l), the presence of symptoms of bilirubin brain damage of any severity and at all stages of the disease, respiratory and cardiac disorders in the absence of data indicating concomitant pneumo- or cardiopathy. In this case, more than two replacement blood transfusions are needed.
Clinical picture- the most severe manifestation of Rh-HDN. A burdened history of the mother is typical - the birth of previous children in a family with HDN, miscarriages, stillbirths, prematurity, transfusions of Rh-incompatible blood, repeated abortions. An ultrasound examination of the fetus is characterized by the pose of the Buddha - the head is at the top, lower limbs bent at the knees and unusually far from the body due to barrel-shaped enlargement of the abdomen, there is a "halo" around the cranial vault.
Due to edema, the mass of the placenta is significantly increased. Normally, the mass of the placenta is 1/6-1/7 of the body weight of the fetus, but with an edematous form, this ratio reaches 1:3 and even 1:1. The villi of the placenta are enlarged, but their capillaries are morphologically immature, abnormal. Characterized by polyhydroamnios. Mothers suffer from severe preeclampsia in the form of preeclampsia, eclampsia.
At birth, the child has the following signs: severe pallor (rarely with an icteric tinge) and general edema, especially pronounced on the external genitalia, legs, head, face; sharply enlarged barrel-shaped abdomen; significant hepato- and splenomegaly (a consequence of erythroid metaplasia in the organs and severe fibrosis in the liver); expansion of the boundaries of relative cardiac dullness, muffled heart sounds; ascites The absence of jaundice at birth is associated with the release of NB from the fetus through the placenta.
After birth, respiratory disorders develop due to hypoplastic lungs or hyaline membrane disease due to an elevated diaphragm in hepatosplenomegaly and ascites. Heart failure develops. Often, children with edematous form of HDN have a hemorrhagic syndrome (bleeding into the brain, lungs, gastrointestinal tract).
From the laboratory data are characteristic: hypoproteinemia (the level of serum protein in the blood falls below 40-45 g / l), an increase in the level of REM in the cord blood (and not just NB), severe anemia (hemoglobin concentration less than 100 g / l), normoblastosis of varying severity and erythroblastosis, thrombocytopenia. The volume of circulating blood is normal and there is no hypervolemia.
Hypoalbuminemia is associated with the leakage of albumin and water from the blood into the interstitium of tissues, although some children may also be deficient in its synthesis by the liver. Most patients do not have a deficiency in albumin synthesis, because as soon as normal diuresis is restored (which happens in survivors on the 2nd-3rd day of life), the level of blood albumin normalizes. One of the pathogenetic factors of ascites, accumulation of fluid in the pleural cavity is considered to be a decrease in drainage function. lymphatic system.
Survivors often develop severe neonatal infections, liver cirrhosis, and encephalopathy.
ICTERUS FORM is the most commonly diagnosed form of HDN. Some children have jaundice already at birth (congenital icteric form), in most children it appears in the first 30 minutes or in the first half of the first day of life. The earlier jaundice appeared, the more severe the course of HDN is usually.
With congenital icteric form, the child has frequent infectious processes (intrauterine or neonatal). In severe postpartum forms of Rh-HDN, jaundice appears in the first 6 hours of life, and in moderate and mild cases, in the second half of the first day of life. With AB0-THN, jaundice appears on the 2-3rd day of life and even later. The intensity and hue of the icteric color gradually change: first orange, then bronze, then lemon, and finally the color of unripe lemon. There is an increase in the liver and spleen, icteric staining of the mucous membranes, and pastosity of the abdomen is often observed.
The appearance of jaundice comes in a certain sequence, since bilirubin begins to be deposited in the proximal part of the body earlier than in the distal - jaundice begins to grow from top to bottom. It is very important to correctly assess the rate and intensity of the increase in jaundice, which makes it possible to differentiate physiological from pathological jaundice.
The degree of jaundice is assessed as severe if jaundice is visible on the first day of life on any part of the body, on the second - on the arms and legs, on the third - on the hands and heels. With an increase in the level of NB in the blood, children become lethargic, adynamic, suck poorly, they have reduced physiological reflexes for newborns, and other signs of bilirubin intoxication appear.
Blood analysis reveals anemia of varying severity, pseudoleukocytosis due to an increase in the number of normoblasts and erythroblasts, often thrombocytopenia, less often a leukemoid reaction. The number of reticulocytes is significantly increased (more than 5‰).
BILIRUBIN ENCEPHALOPATHY(BE) is rarely clinically detected in the first 36 hours of life, and usually its first manifestations are diagnosed on the 3-6th day of life. Four phases of the course of BE are characteristic:
1) dominance of signs of bilirubin intoxication - lethargy, decreased muscle tone and appetite up to refusal of food, "poverty" of movements and emotional coloring of the cry (monotonous, unemotional), incomplete expression of the Moro reflex (there is only its first phase), rotational nystagmus, regurgitation, vomiting, pathological yawning, "wandering look";
2) the appearance of classic signs of nuclear jaundice - spasticity, stiff neck, forced position of the body with opisthotonus, stiff limbs and clenched hands; periodic excitation and a sharp "brain" high-frequency cry, bulging of a large fontanelle, twitching of the muscles of the face or complete amimia, large-scale tremor of the hands, convulsions; symptom of "setting sun"; the disappearance of the Moro reflex and the visible reaction to a strong sound, the sucking reflex; nystagmus; respiratory arrest, bradycardia, lethargy, sometimes fever (fever or hyperthermia); progressive deterioration neurological symptoms(usually lasts for a day);
3) a period of false well-being and the disappearance of spasticity (starting from the middle of the 2nd week of life), when it seems that the reverse development of neurological symptoms will even lead to an almost complete rehabilitation of the child;
4) formation period clinical picture neurological complications begin at the end of the neonatal period or at the 3-5th month of life: athetosis, choreoathetosis, paralysis, paresis; deafness; cerebral palsy; delay mental development; dysarthria.
A lethal outcome as a consequence of brain damage is possible both in the first and second phases of BE and is observed against the background of the appearance of hemorrhagic syndrome, disorders of cardiac activity and respiration. At the same time, it was noted that in newborns, especially premature ones, with kernicterus diagnosed in the section, its classical signs were not always clinically expressed.
In the first phase of BE, brain damage is reversible. But, unfortunately, all clinical symptoms of the first phase of BE are nonspecific, and therefore instrumental approaches to its diagnosis are being developed.
ANEMIC FORM diagnosed in 10-20% of patients. Babies are pale, somewhat lethargic, suckle poorly, and put on weight. They find an increase in the size of the liver and spleen, in the peripheral blood - anemia of varying severity in combination with normoblastosis, reticulocytosis, spherocytosis (with ABO conflict). Sometimes hyporegenerative anemia is observed, without reticulocytosis and normoblastosis, which is explained by inhibition of bone marrow function and a delay in the release of immature and mature forms of erythrocytes from it. NB levels are usually normal or moderately elevated. Signs of anemia appear at the end of the first or even the second week of life. In some cases, anemia first develops at the 3rd week of life and under the influence of external factors - infectious diseases, the appointment of certain medications (sulfonamides, nitrofurans, nalidoxic acid, paracetamol, vitamin K, acetylsalicylic acid, antihistamines, chloramphenicol, tetracycline, apilac, thiazides ), against the background of natural feeding (a potential source of isoantibodies), which can lead to a sharp increase in hemolysis and even the development of decompensated DIC. In such patients, under the influence of antibodies, the activity of glucose-6-phosphate dehydrogenase of erythrocytes and glutathione reductase is persistently reduced.
Course and prognosis of HDN depends on the form and severity of the disease, the timeliness and correctness of treatment.
With edematous form, the prognosis is often unfavorable.
The prognosis for life in most children with icteric form of the disease is favorable. It is necessary to remember the phase of false well-being in BE, and all children with hyperbilirubinemia more than 343-400 µmol/l should be sent to neurological department for newborns or under the supervision of a neurologist for rehabilitation measures, if they had only signs of bilirubin intoxication, i.e. first phase of BE. In 5-30% of patients with hyperbilirubinemia 257-342 µmol/l, psychomotor development retardation, asthenic syndrome, neuroses and other abnormalities in the neuropsychic status are noted in the future. Active neurotrophic therapy of such patients, started in the neonatal period, significantly improves the long-term neurological prognosis. In children who have had icteric form of HDN, there is a high infectious morbidity in the first year of life.
The course of ABO-HDN is usually milder than RH-THN: there is practically no edematous form, more often there is anemic and mild and moderate icteric forms. However, with ABO-THN, the development of intravascular hemolysis with decompensated DIC, kernicterus is possible.
In the early neonatal period in children with TTH, the most frequent complication is hypoglycemia, more rare are edematous, hemorrhagic, cardiopathic syndromes and "bile thickening" syndrome.
At the age of 1-3 months, children who have received an exchange transfusion due to HDN may develop normochromic, hypo- or normoregenerative anemia due to temporary insufficient activity of the erythropoietic function of the bone marrow, vitamin E and iron deficiency. In this regard, from the 3rd week, it is advisable to prescribe exogenous erythropoietin (for example, epocrine), a prophylactic dose of iron preparations (2 mg / kg / day) to children who have had TTH. Vitamin E should be prescribed only with proven deficiency.
Diagnosis. HDN is suspected when:
HDN in previous children in the family;
Jaundice that appeared on the first day of life;
Rh-negative and / or O (I) mother and Rh-positive and / or A (II), B (III), AB (IV) belongings of the child;
The rise in the level of bilirubin is more than 9 µmol / l / hour;
Inefficiency of phototherapy;
Pseudohyperleukocytosis in a child (due to an excess of erythroid nuclear forms);
The child has anemia, pallor and / or hepatosplenomegaly.
Severe HDN can be diagnosed prenatally. In all women with Rh-negative blood, the titer of anti-Rh antibodies is examined at least three times. The first study is carried out when registering with a antenatal clinic. It is optimal to further conduct a second study at 18-20 weeks, and in the third trimester of pregnancy, it should be done every 4 weeks. Of great value is the determination of the level of bilirubin in the amniotic fluid.
If the titer of Rh antibodies is 1:16-1:32 or more, then amniocentesis is performed at 26-28 weeks and the concentration of bilirubin-like substances in the amniotic fluid is determined. If the optical density with a 450 mm filter is more than 0.18, an intrauterine exchange transfusion is usually necessary. It is not carried out on fetuses older than 32 weeks of gestation. 2-3 weeks before the expected birth, it is necessary to assess the maturity of the lungs, and if they are immature, prescribe dexamethasone or betamethasone to the mother.
Prognostically unfavorable is the "jumping" titer of Rh antibodies in a pregnant woman; in this case, severe icteric forms of HDN develop more often.
The method of diagnosing the congenital edematous form is also an ultrasound examination, which reveals the edema of the fetus. It develops with a deficiency of hemoglobin levels of 70-100 g / l. In this case, cordocentesis is performed using fetoscopy, the level of hemoglobin in the child is determined and, according to indications, the red blood cell mass is transfused or an exchange transfusion is performed. important differential diagnosis with non-immune forms of fetal edema.
Survey plan for suspected HDN:
1. Determination of the blood group and Rh affiliation of the mother and child.
2. Analysis of the peripheral blood of the child with an assessment of the blood smear.
3. Blood test with counting the number of reticulocytes.
4. Dynamic determination of the concentration of bilirubin in the child's blood serum.
5. Immunological studies.
Changes in the peripheral blood of the child: anemia, hyperreticulocytosis, pseudoleukocytosis due to an increased amount of nuclear forms of the erythroid series in the blood.
Immunological studies. In all children of Rh-negative mothers, the blood group and Rh-affiliation, serum bilirubin level are determined in the cord blood.
In case of Rh incompatibility, the titer of Rh antibodies in the mother's blood and milk is determined, as well as the direct Coombs reaction with the child's erythrocytes and the indirect Coombs reaction with the mother's blood serum, the dynamics of Rh antibodies in the mother's blood during pregnancy and the outcome of previous pregnancies are analyzed.
With ABO incompatibility, the titer of allohemagglutinins (to the erythrocyte antigen present in the child and absent in the mother) is determined in the mother’s blood and milk, in protein (colloidal) and salt media, in order to distinguish natural agglutinins (they have a large molecular weight and belong to immunoglobulins class M, do not cross the placenta) from immune (these agglutinins have a small molecular weight, belong to class G immunoglobulins, which easily cross the placenta, and after birth - with milk, i.e. responsible for the development of HDN). In the presence of immune antibodies, the titer of allohemagglutinins in the protein medium is two steps or more (i.e., 4 times or more) higher than in the salt medium.
Direct Coombs' test with AB0-conflict in a child, as a rule, is weakly positive, i.e. a slight agglutination appears after 4-8 minutes, while with a Rh conflict, agglutination is noticeable after 1 minute.
Plan for further laboratory examination of the child includes regular determination of the level of glycemia (at least 4 times a day in the first 3-4 days of life), NB (at least 2-3 times a day until the level of NB in the blood begins to decrease), plasma hemoglobin (on the first day and beyond according to indications), platelet count, transaminase activity (at least once) and other studies, depending on the characteristics of the clinical picture.
TREATMENT OF HDN
Treatment in the antenatal period. With an antenatal diagnosis of the edematous form of HDN, an erythrocyte mass is transfused into the umbilical cord vein of an intrauterine fetus after cordocentesis or an exchange transfusion (EBT). Babies born alive after intrauterine FRD may not have anemia at birth, but will require repeated FRD after birth due to severe hyperbilirubinemia.
Treatment after birth The main methods of treating TTH are phototherapy (PT) and exchange transfusion (BRT). Other methods of treatment (phenobarbital) are significantly inferior in their effectiveness or are in the stage of clinical testing (metaloporphyrins). Depending on the degree of hyperbilirubinemia, the rate of increase in the concentration of bilirubin, the age and maturity of the child, it is determined which method should be used - phototherapy or exchange transfusion.
At CONGENITAL EDEDEMATIC FORM OF HDN it is necessary to immediately (within 5-10 seconds) clamp the umbilical cord, because the delay can stimulate the development of hypervolemia. Thermal protection, urgent (within an hour) onset of PPC, or red blood cell transfusion are needed if children are not icteric. Heart failure is not present at birth, but it develops easily after birth. In this regard, at first, the erythrocyte mass is transfused in a volume of only 10 ml, and during the first PPC (Rh-negative erythrocyte mass suspended in fresh frozen plasma with a hematocrit of 0.7), its total volume sometimes decreases to 75-80 ml / kg or, if the PKK is carried out in full (170 ml / kg), then 50 ml more blood is released than is injected. Transfusion is carried out very slowly. As a rule, repeated FPCs are necessary.
Taking into account the presence already at birth of respiratory disorders due to lung hypoplasia or hyaline membrane disease, additional oxygen supply with the creation of positive pressure at the exit or mechanical ventilation is necessary. The presence of hemorrhagic syndrome requires a transfusion of fresh frozen plasma, with severe thrombocytopenia (less than 30,000 per 1 μl) transfusion of platelet mass is indicated, with very severe hypoproteinemia (less than 40 g / l) - 12.5% albumin solution (1 g / kg), with the development heart failure - prescribing digoxin (saturation dose of 0.02 mg / kg is given in 2-3 days). On the 2-3rd day of life, furosemide is sometimes prescribed.
At ICTERUS FORM HDN feeding begins 2-6 hours after birth, it is carried out with donor milk in an amount corresponding to age, until the disappearance of isoantibodies in mother's milk, which usually happens at the 2nd week of life.
If the next day after the child is twice attached to the mother's breast, the level of NB and reticulocytosis in his blood do not increase, breastfeeding is allowed. It should be remembered that if the mother does not breastfeed for some time, everything must be done to maintain lactation (the mother must carefully express milk). After pasteurization, it can also be given to her child with HDN.
The treatment of hyperbilirubinemia itself with NB in the blood is divided into conservative and operative (blood exchange transfusion, plasmapheresis, hemosorption).
PHOTO THERAPY - completely safe and effective method treatment. The positive effect of phototherapy is to increase the excretion of bilirubin from the body with feces and urine, reduce the toxicity of NB and the risk of kernicterus in high indirect hyperbilirubinemia. Under the influence of light at a depth of 2 mm of the skin, three chemical reactions occur:
1) Photooxidation - photooxidation of NB with the formation of biliverdin, dipyrroles or monopyrroles, which are water-soluble and excreted from the body with urine and feces (washed out yellow blood plasma);
2) Configurational isomerization of the NB molecule, which becomes water-soluble (occurs most rapidly, but is reversible in the dark);
3) Structural isomerization of the NB molecule with the formation of lumibirubin, which is excreted in the unconjugated form with bile and urine. The duration of its half-life from the blood is 2 hours, while unchanged HB is 12-15 hours.
The effectiveness of phototherapy is determined by four facts:
1) The wavelength of the light source. Special blue fluorescent light lamps are most effective because bilirubin is absorbed most in the blue light region (between 420 and 500 nm). Tungsten halogen lamps are also used.
2) Illumination. Typically, the light source is placed at a distance of 15-20 cm above the child, and the irradiation should not be less than 5-6 μW/cm 2 /nm. The best effect is achieved at an illumination of 10-11 μW/cm 2 /nm. This can be achieved with a combination of 4 daylight and 4 blue light bulbs of 20W each.
3) The size of the irradiated surface. The larger the radiation surface, the more effective phototherapy. Therefore, the child should be completely naked (only the eyes and genitals are covered, although the damaging effect of phototherapy on the sex glands has not been established). To increase the effectiveness of phototherapy, fiber-optic phototherapy is used - special "luminous" mattresses, blankets, inside of which there are diodes of halogen lamps.
4) Constancy or discontinuity. It is believed that phototherapy should be carried out continuously, but a break of about 1 hour after a 6-12 hour exposure does not reduce its effectiveness. Short breaks are taken during feeding and communication between the child and the family.
Thus, several modes of phototherapy are used:
Continuous FT - continuously for 24 hours, usually used for severe hyperbilirubinemia, premature babies.
Intermittent FT - breaks are made for feeding and procedures.
"Double" PT - PT of increased intensity, when the child is placed in a special chamber in which PT lamps are located on all sides or the child is illuminated from both sides using a lamp and a luminous mattress. This type of PT is the most effective and is used in the most severe cases or in combination with ZPK.
For full-term newborns, phototherapy is started at the level of NB in the blood of 205 µmol/l or more, and for premature babies - about 171 µmol/l. In very low birth weight infants, phototherapy is initiated at a serum NB level of 100–150 µmol/L. It is highly desirable to start phototherapy within the first 24-48 hours of life.
Side effects of phototherapy can include:
1. Greater than normal, imperceptible water loss (by 50% if a heat shield is not used, and by 10-20% when using a plastic heat shield, i.e. with phototherapy of a child in an incubator), so children should receive additional 10-15 ml of liquid per 1 kg of body weight per day.
2. Diarrhea with green stools determined by NB photoderivatives; does not require treatment.
3. Transient eruptions on the skin, some lethargy and distension of the abdomen; therapy is not required.
4. The “bronze child” syndrome (blood serum, urine and skin are colored in bronze) occurs exclusively in children with high levels of REM and liver damage. It is believed that some derivatives of bile pigments give this color. The skin returns to its normal color after a few weeks, and the child's prognosis is determined by the severity of liver damage. Phototherapy is not indicated for children with high REM levels.
5. Tendency towards thrombocytopenia due to increased platelet turnover.
6. In children with very low birth weight, on the background of phototherapy, there is an increase in the frequency of persistent ductus duct syndrome.
7. Transient deficiency of riboflavin with prolonged phototherapy; the addition of riboflavin to the treatment of children receiving phototherapy does not increase the effectiveness of the latter.
The usual duration of phototherapy is 72-96 hours, but it can be less if the level of NB has reached the physiological age for the child.
Phototherapy is more effective when combined with INFUSION THERAPY. On the first day of life, 50-60 ml/kg of a 5% glucose solution is usually infused, then 20 ml/kg is added daily, and by the 5th day the volume is brought to 150 ml/kg, taking into account the volume of enteral nutrition and weight loss of the child over the previous day . From the second day of life, for every 100 ml of 5% glucose solution, add 1 ml of 10% calcium gluconate solution, 2 mmol of sodium and chlorine (13 ml of isotonic sodium chloride solution). Infusion rate - 3-4 drops per 1 minute. The addition of albumin solutions is indicated only with proven hypoproteinemia.
CLEANING ENEMAS in the first 2 hours of life or suppositories with glycerin, delivered at the same time, leading to an early discharge of meconium, significantly reduce the severity of the maximum rise in the level of blood NB. These activities should be carried out in all children with jaundice at birth. However, after 12 hours of life, such treatment has no effect.
PHENOBARBITAL, prescribed after birth, helps to activate the formation of REM, improve the outflow of bile and, accordingly, reduce the intensity of jaundice. However, this effect is distinct only on the 4-5th day of therapy. To do this, on the first day of therapy, phenobarbital is prescribed at a dose of 20 mcg / kg / day (divided into 3 doses) and then 3.5-4.0 mg / kg per day.
Antenatal treatment with phenobarbital is carried out for pregnant women at a dose of 100 mg per day (in 3 divided doses) 3-5 days before delivery. If childbirth has not occurred, then 100 mg of phenobarbital is given 1 time per week. But side effects are possible, among which there is an increased frequency of hemorrhagic syndrome, hyperexcitability, the use of phenobarbital can lead to a deficit of neurons, developmental disorders of the reproductive system.
ANTI-RH-IMMUNOGLOBULINS for intravenous administration. Usually a single dose of 0.5 kg/kg of body weight is sufficient as soon as the diagnosis is made. However, there is an opinion about the advisability of repeated administration at the same dose after 48 hours. Serious side effects of such therapy in the neonatal period are very rare.
REPLACEMENT BLOOD TRANSFUSION. Indications for PPC in the treatment of HDN:
The concentration of bilirubin in the blood of the vein of the umbilical cord is more than 85 µmol / l;
The concentration of bilirubin is more than 340 µmol / l at any age;
An increase in the concentration of bilirubin over 8.5 µmol/l/hour;
With HDN for ABO antigens - an increase in the concentration of bilirubin over 17 μmol / l / h, despite the ongoing phototherapy;
Anemia (hematocrit less than 45%, hemoglobin 110-130 g/l);
Clinical manifestations of nuclear jaundice, regardless of age;
The appearance of jaundice or severe pallor of the skin in the first hours of life in a child with an increase in the size of the liver or spleen
If the newborn has risk factors - prematurity, sepsis, hypoxia, acidosis, hypoproteinemia - FPC is performed at lower concentrations of bilirubin in the blood.
To determine the approximate limits of the concentration of bilirubin, at which ZPK should be carried out, you can use the formula: bilirubin concentration (µmol/l) = gestational age (in weeks) x 10.
The choice of treatment method depending on the concentration of bilirubin in blood plasma (µmol/l)
Carrying out the FPC contributes to the removal of bilirubin, the replacement of sensitized erythrocytes of the newborn, the removal of antibodies from the circulation and the elimination of anemia.
In case of Rh-conflict, blood of the same group as that of a child (Rh-negative) is used for ZPK, no more than 2-3 days of conservation in the amount of 160-170 ml / kg, in case of group - group IV plasma and erythrocytes 0 (I ) groups, and in this case, the FPC is carried out in full - 170-180 ml / kg. Mixing two blood components doubles the risk of transmission of viral infections (not only hepatitis and HIV, but also cytomegaloviruses and other herpes viruses). If for full-term children with HDN the risk of these infections is not so great, then for children weighing less than 1.5 kg it poses a real threat, and therefore it is still better for them to carry out TRP with whole blood, and preferably after checking it not only for hepatitis, HIV, syphilis, but also on cytomegaly.
The following points should be kept in mind when conducting a PPP:
The tip of a properly placed umbilical venous catheter should be in the vena cava between the diaphragm and the left atrium; the length of the umbilical venous catheter from its end to the mark at the level of the umbilical ring is equal to the distance from the shoulder to the navel - 5 cm, but it can be more accurately determined by a special nomogram;
Many clinics believe that transfused blood should be heated to 35-37°C (at the same time, overheating of the blood is extremely dangerous!); before the start of the ZPK, the gastric contents are aspirated;
The procedure begins with the removal of 30-40 ml (in premature babies - 20 ml) of the child's blood; the amount of injected blood should be 50 ml more than the output (for polycythemia, the same amount is infused as is withdrawn);
The operation should be carried out slowly - 3-4 ml per minute with alternating excretion and administration of 20 ml of blood (in premature babies - 10 ml); the duration of the entire operation is at least 2 hours;
For every 100 ml of injected blood, 1 ml of a 10% calcium gluconate solution should be injected.
The level of bilirubin is determined in the child's blood serum before and immediately after the ZPK. After the operation, a urine test is necessary, and after 1-2 hours - a determination of the level of glucose in the blood.
Complications of PPC: 1. Cardiac: a) acute heart failure with the rapid introduction of large amounts of blood and the development of hypervolemia, volume overload;
b) cardiac arrhythmias and cardiac arrest due to hyperkalemia, hypocalcemia or excess citrate in the blood.
2. Vascular: a) air emboli (due to negative pressure in the umbilical vein with active blood suction and other technical violations - a small diameter of the catheter and a wide vein, which can lead to air penetration between the walls of the vessel and the catheter);
b) thrombosis of the portal vein due to vascular injury with a catheter, hyperviscosity;
c) vessel perforation.
3. Infectious - viral, protozoal and bacterial infections (sepsis, cytomegaly, hepatitis B and C, HIV infection).
4. Ulcerative necrotic enterocolitis without or with intestinal perforation (due to ischemia).
5. Anemia (mechanical, thermal injury of erythrocytes, hemolysis by alloantibodies).
6. Hemorrhagic syndrome due to thrombocytopenia, deficiency of procoagulants, excessive heparinization, vessel perforation.
7. Metabolic (hypoglycemia, acidosis, hyperkalemia, hypocalcemia, hypomagnesemia).
8. Hypothermia.
9. Transfusion complications with intravascular hemolysis due to improper selection of donor blood (fever, hematuria, acute renal failure, shock).
10. Graft-versus-host reaction.
The strictest observance of asepsis and antiseptics is a necessary condition for carrying out PKK (in particular, antibiotics are prescribed within 2-3 days after PKK, usually ampicillin).
After PKK, conservative therapy is mandatory - phototherapy, infusion therapy to treat or prevent hypoglycemia. Enteral nutrition begins after 6-8 hours. The level of NB in the blood serum is determined after 8-12 hours. After PKD, the level of bilirubin in the blood rises due to its release from the tissues, therefore, indications for repeated PKD are determined by the indicators of NB in serum no earlier than 12 hours later. The growth rate of NB is more than 6 µmol/hour - an indication for repeated PPC. Hemosorption and plasmapheresis are carried out according to the same indications as ZPK. Plasmapheresis is contraindicated in thrombocytopenia.
Late anemia in children with HDN is hypoerythropoietic and hyporegenerative in nature, and therefore requires treatment with recombinant erythropoietin at a dose of 200 IU/kg 3 times a week (a course of 10 injections of the drug) from the 2-3rd week of life in combination with iron preparations (elemental iron 2 mg/kg/day).
Forecast. Perinatal mortality in TTH in the 1940s was 40-45%, by the end of the 20th century it had decreased to 2.5%.
Prevention. Each girl should be considered as a future mother and blood transfusion should be carried out only for health reasons. In the prevention of HDN, an important place is given to the work to explain to women the harm of abortion.
All women with Rh-negative blood affiliation should be given anti-D-globulin (250-300 μg) on the first day after childbirth or abortion, which promotes the rapid elimination of the child's red blood cells from the mother's bloodstream, preventing the synthesis of Rh antibodies by the mother.
For women with a high titer of Rh antibodies in the blood during pregnancy, for the prevention of HDN, husband's skin grafting is done (a 2 x 2 cm flap in the axillary region); at 16-32 weeks of pregnancy 2-3 times with an interval of 4-6-8 weeks. Plasmapheresis is performed (plasma removal with Rh antibodies and the introduction of red blood cells back). At the 37-39th week, the pregnancy is delivered by caesarean section.
Pregnant women with a high titer of anti-Rhesus antibodies are hospitalized for 12-14 days in the antenatal department at 8, 16, 24, 28 and 32 weeks; non-specific treatment is also carried out: intravenous infusions of glucose with ascorbic acid, cocarboxylase, rutin, vitamins E, B 6, calcium gluconate, oxygen and anti-anemic therapy are prescribed, and if there is a threat of miscarriage - progesterone, endonasal electrophoresis of vitamins B1, C.
3-5 days before delivery, the appointment of phenobarbital 0.1 g orally 3 times a day is indicated.
Prevention of severe forms of HDN after birth is also intrauterine exchange transfusion of blood in edematous forms.
APLASTIC ANEMIA IN CHILDREN
Aplastic anemia (AA)– a disease characterized by peripheral pancytopenia, a decrease in the number of hematopoietic cells in the bone marrow with the replacement of cellular hematopoiesis with adipose tissue, without signs of blast transformation, an increase in the organs of the reticuloendothelial system (liver, spleen, lymph nodes); bone marrow failure (inability to produce the required amount of blood cells per unit of time). In pancytopenic forms, megakaryocytes and myelocytes are absent. Code D 60-64 (ICB-10).
The prevalence of AA is 2-6 per 1 million population, most often occurs at the age of 0-20 years.
Etiopathogenesis. AA can develop after the action of certain factors that have a toxic effect on the human bone marrow, of chemical and physical origin.
Chemical agents include gasoline, benzene and its derivatives, bismuth preparations, mercury vapor, acids, dyes, heavy metal compounds (gold salts), organic arsenic and others. In the emergence of AA possible cause there may be drugs: levomycetin (chloramphenicol), amidopyrine and other analgesics and antipyretics, sulfonamides, streptomycin, tetracycline, barbiturates, cytostatics and others. The effect of these chemicals affecting bone marrow hematopoiesis is associated by researchers with dosage toxicity or with idiosyncrasy.
Among the physical factors, first of all, include ionizing radiation, which has a penetrating effect and causes the death of stem cells.
It is believed that AA in children can develop after exposure to viruses such as parvovirus, the AIDS virus, viruses that cause hepatitis, and others.
From the foregoing, it follows that AA is a polyetiological disease, in the occurrence of which not only the causal factor plays a role, but the individual reactivity of the organism. Hereditary factors are also of undoubted importance, as evidenced by the existence of hereditary forms of AA in nature.
It should be noted that in children only in 10-20% of cases it is possible to establish a specific cause of the disease, in other cases the factor leading to impaired hematopoiesis is unknown (such forms of AA are called idiopathic ).
Pathogenetic mechanisms occurrence of AA require further study. At the present stage, AA is considered as a disease based on damage to hemocytopoiesis at the level of the earliest precursors of hemocytes, possibly even stem cells. This assumption is based on the fact of inhibition of all hematopoietic sprouts and an increase in the content of endogenous hemocytopoietins. Of no small importance in the occurrence of AA is also the defeat of the hematopoietic stroma, which creates the microenvironment of stem cells and is a regulator of the processes of proliferation and differentiation.
It has been established that the main functional defect of hematopoiesis is a violation of proliferation processes. At the same time, disturbances in intracellular metabolism occur, and the process of maturation of hemocytopoietic cells is lengthened. When assessing ineffective erythrocytopoiesis, the accumulation of cells at the early stages of differentiation was noted. Consequently, AA disrupts the processes of nucleic acid synthesis, which leads to inhibition of proliferation and differentiation of hemocytes. Along with erythropoiesis, leukocytopoiesis and thrombocytopoiesis suffer.
Thus, modern studies have identified several mechanisms for the development of AA:
* quantitative deficiency and qualitative defects of stem cells;
* immunological suppression of hematopoiesis;
* violation of the microenvironment of stem cells, changing their function;
* external humoral or cellular (immune) influences that disrupt the normal function of stem cells.
According to AI Vorobyov, a significant part of AA (especially acquired forms) is caused by immunological disorders (antibodies that destroy stem cells begin to be produced in the body).
Classification. Proposed by V.I. Kalinicheva (1983), suggests the division of AA into two large groups: hereditary and acquired forms.
hereditary AA.
I. Hereditary AA with a general lesion of hematopoiesis.
1. Hereditary AA with a general lesion of hematopoiesis and congenital malformations (constitutional Fanconi anemia).
2. Hereditary familial AA with a general lesion of hematopoiesis without congenital developmental anomalies (Estrena-Dameshek anemia).
II. Hereditary partial AA with selective damage to hematopoiesis (Diamond-Blackfan anemia).
Acquired by AA.
I. With a general lesion of hematopoiesis.
1. Acute acquired AA.
2. Subacute acquired AA.
3. Chronic acquired AA.
II. Partial acquired AA with selective damage to hematopoiesis.
According to international criteria for assessing the severity of AA, there are three groups:
1) Super severe form: in the peripheral blood of patients, deep pancytopenia is detected with a rapid and sharp decrease in granulocytes to single cells in blood smears.
2) Severe form: indicators of peripheral blood also indicate a deep inhibition of hematopoiesis. The content of granulocytes is less than 0.5 x 10 9 /l, reticulocytes - less than 1‰, the number of myelokaryocytes - less than 40 x 10 9 /l. Non-myeloid cells - more than 50%. Bone marrow punctate: signs of relatively intact hematopoiesis in the form of proliferating elements of granulocytic and erythroid germs.
3) The mild form is characterized by a less profound inhibition of hematopoiesis. The number of granulocytes is above 0.5 x 10 9 /l, reticulocytes - more than 1‰. Along with areas of reduced cellularity of the bone marrow, normocellular foci are found, while the number of non-myeloid cells is less than 50%, and erythroid cells are normal or increased.
Clinical symptoms AA, regardless of form, consists of several syndromes:
1. Anemic syndrome (pallor of the skin and mucous membranes, general weakness, increased fatigue).
2. Hemorrhagic syndrome (skin hemorrhages, bleeding from the nose, gums, urinary tract, and others).
3. Infectious complications (pneumonia, sepsis, otitis, sinusitis, gingivitis, urinary infection, and others).
4. Intoxication syndrome (fever, sweating).
Hepatosplenomegaly and lymphadenopathy are not typical for patients with AA.
feature Fanconi constitutional anemia is that in most cases it has a family character (the type of inheritance is autosomal recessive, not related to sex). The proof of the genetic basis of the disease is the detection of chromosome changes in the culture of peripheral blood lymphocytes (chromatid exchange, chromatid breakdown, endoreduplication).
With Fanconi anemia, pancytopenia does not appear until 4-7 years of age. Parents complain of the child's pallor from birth, constantly reduced appetite, sometimes dyspeptic symptoms, low mobility and isolation. Against this background, symptoms of bleeding sometimes appear. Body temperature is normal, in the presence of hidden foci of infection - subfebrile. With the addition of intercurrent diseases or in the terminal period, high fever is observed.
All patients with Fanconi anemia have congenital developmental anomalies - microcephaly, strabismus, ptosis, nystagmus, multiple hyperpigmentations on the body, anomalies auricles, deafness, hearing loss, deformations of the bone skeleton (aplasia and hypoplasia thumb on the arms, polydactyly or syndactyly, dysplasia hip joints etc.), anomalies of the kidneys and urinary tract, hypospadias, cryptorchidism, congenital heart defects, mental retardation, short stature, lag of bone age by 2-5 years, increased tendon reflexes.
In the hemogram - pancytopenia, macrocytic hyperchromic (or normochromic) anemia, little or no reticulocytes, toxic neutrophil granularity, relative lymphocytosis, ESR is accelerated. Bleeding time is prolonged (hypocoagulation). Serum iron normal or elevated.
The course of Fanconi anemia is chronic, with a gradual onset, with periods of exacerbation and remissions, steadily progressing. The prognosis is unfavorable, life expectancy is from 1 to 8 years, the cause of death is profuse bleeding and infectious complications. Hemotransfusion dependence is characteristic.
Diamond-Blackfan anemia characterized by a selective lesion of the erythrocyte germ.
It has now been established that this disease is associated with a genetic defect in stromal fibroblasts, in particular, genes responsible for the synthesis of stem cell growth factor and its receptor.
Starts at early age, gradually, in the first months of life, progressive pallor, weakness, lethargy appear. The child lags behind in physical and motor development. There may be dyspeptic disorders, often a secondary infection joins. There is no bleeding in this form of AA.
Unlike Fanconi anemia, Diamond-Blackfan anemia does not cause pancytopenia. The disease is manifested mainly by anemic syndrome. As a rule, anemia is pronounced, has a normochromic normocytic character with reticulocypenia. In the myelogram, starting from the early stages of the development of the process, there is a sharp decrease in the number of elements of the erythroid germ, with completely intact white and platelet germs.
The prognosis of the disease is now improving and with early treatment is relatively favorable. With systematic blood transfusions, children live up to 15 years, after which spontaneous improvement occurs. However, systematic blood transfusions lead to tissue hemosiderosis.
Acquired by AA more common at school age. Most children before the disease are considered healthy. Acute, subacute and chronic acquired AA are distinguished along the course.
Acute acquired AA is characterized by a sudden onset and a rapid progressive course, a pronounced hemorrhagic syndrome and septic-necrotic phenomena. Signs of general intoxication are rapidly growing. Within a few months, the disease progresses rapidly.
Subacute acquired AA begins gradually - pallor of the skin, general weakness, malaise, headache, dizziness, and undulating fever are noted. The face becomes puffy, the limbs become pasty. Ecchymosis and petechiae appear on the skin, they are joined by nasal and gingival bleeding. Girls in puberty may have uterine bleeding.
Chronic acquired AA is characterized by a long course. The disease develops gradually. Most early signs are gradually increasing weakness, fatigue, loss of appetite, pale skin with a waxy tint. The temperature is subfebrile. Hemorrhagic syndrome and necrotic skin lesions are observed very rarely and will join only in the terminal stage of the disease.
In all variants of acquired AA, peripheral The lymph nodes, liver and spleen are usually not enlarged. In the advanced stage of the disease, the expansion of the borders of the heart to the left, deafness of tones, systolic murmur, tachycardia, arterial hypotension are determined. From the side digestive system typical complaints of abdominal pain, vomiting, sometimes gastrointestinal bleeding.
Forecast when acquired AA in children is serious, the survival rate is 10-20%.
Diagnostics AA is based on the results of clinical laboratory and instrumental studies.
Pancytopenia is a pathognomonic sign of AA. A deeper form of pancytopenia occurs in severe and super-severe AA. At the same time, there are no signs of regeneration, leukopenia develops due to neutropenia in combination with relative lymphocytosis, in some patients - absolute lymphocytosis. A characteristic feature of leukopenia is its persistence even with the addition of a secondary infection. An important symptom is thrombocytopenia. AA is almost always accompanied by a significant acceleration of erythrocyte sedimentation.
Peripheral blood parameters:
* absolute number of granulocytes< 1,5 тыс. в 1 мкл;
* platelet count< 150 тыс. в 1 мкл;
* number of reticulocytes< 5% (после коррекции);
* hyperchromic (normochromic) macrocytic anemia;
* hypersiderinemia;
* Relative lymphocytosis.
Bone marrow: the pathological process in AA develops unevenly, gradually capturing all the flat bones, including the sternum. Trepanobiopsy ilium in the diagnosis of AA, in addition to exceptional diagnostic advantages, it provides a detailed description of bone marrow hematopoiesis, the ability to make predictions and monitor the effectiveness of treatment. Characteristic features:
* reduced cellularity (myelokaryocytes 100 thousand< в 1 мкл, мегакариоциты < 40 в 1 мкл);
* Decreased proliferation and differentiation of erythroid cells;
* absence of blast cells;
* replacement of cellular hematopoiesis with adipose tissue (according to trepanobiopsy);
* development of "nesting" of bone marrow hematopoiesis (according to trepanobiopsy).
Similar information.
The occurrence of an immune conflict underlying hemolytic disease of the newborn is possible if the mother is antigen-negative and the fetus is antigen-positive. With the development of GBPiN by the Rh factor, the erythrocytes of the mother are Rh-negative, and the fetus is Rh-positive, i.e. contain the O factor. Realization of the conflict (development of GBPiN) is usually carried out during repeated pregnancies, since previous sensitization is necessary.
Hemolytic disease of the newborn due to group incompatibility develops with 0 (1) blood type in the mother and A (II) or, less commonly, B (III) blood group in the fetus. Realization of the conflict is possible already during the first pregnancy. GBPiN can also occur with incompatibility for other rare antigenic systems: Kell, Lutheran, etc.
How does hemolytic disease of the newborn develop?
For the development of hemolytic disease of the newborn, antigen-positive fetal erythrocytes must enter the bloodstream of an antigen-negative pregnant woman. At the same time, it is not so much the fact of the transplacental transfer of fetal erythrocytes that is of great importance, but the amount of fetal blood that enters the mother's body. The factors contributing to isoimmunization, especially by the Rh factor, include:
- previous medical and non-medical abortions;
- previous spontaneous (one or more) miscarriages;
- previous ectopic pregnancy;
- previous births (premature and urgent);
- invasive diagnostic methods(amniocentesis, cordocentesis, chorionbiopsy);
- threat of abortion.
The basis of the disease is hemolysis (destruction) of erythrocytes, due to the incompatibility of the blood of the mother and fetus according to the Rh factor, group and other blood factors, which occurs at 3-4 months of intrauterine development and increases sharply after birth.
When antigen-positive fetal erythrocytes enter the bloodstream of an antigen-negative woman, anti-Rhesus or group antibodies are produced in her body. If the antibodies belong to the IgG class, then they pass transplacentally into the fetal circulation, bind to antigen-positive erythrocytes of the fetus, causing their hemolysis.
The Rh antigen system consists of six main antigens: C, c, D, d, E and e. Rh-positive erythrocytes contain D-factor, and Rh-negative erythrocytes do not contain it, although other antigens of the Rh system are often found in them. The Rh-negative pregnant fetal erythrocytes that have penetrated into the bloodstream of the fetus, which have a D-antigen, lead during the first pregnancy to the synthesis of Rh-antibodies related to class M immunoglobulins that do not cross the placenta. Then class G immunoglobulins are produced that can overcome the placental barrier. Due to the low number of fetal erythrocytes and immunosuppressive mechanisms, the primary immune response in a pregnant woman is reduced. That is why the implementation of the conflict with Rh incompatibility during the first pregnancy practically does not occur, and the child is born healthy. With repeated pregnancies, the development of a conflict is possible, and the child is born with hemolytic disease of the newborn.
A- and B-antigens are located on the outer surface of the plasma membrane of the erythrocyte. Isoimmune anti-A and anti-B group antibodies belong to the IgG class, in contrast to natural group antibodies - calamus, which belong to class IgM. Isoimmune antibodies can combine with the corresponding antigens A and B and be fixed on other tissues, including those of the placenta. That is why hemolytic disease of the newborn according to the ABO system can develop already during the first pregnancy, but only in about 10% of cases.
If it is possible to implement both variants of the conflict, a conflict occurs more often according to the AB (0) system.
But not only the Rh factor is the cause of the development of the disease. It can occur with blood incompatibility and other factors. In addition, hemolytic disease of the fetus can occur when the blood of the mother and fetus does not match the main blood groups of the AB0 system. Antigens A and B, inherited from the father, can cause the formation of incomplete agglutinins in a mother with blood type 0, which, unlike normal α- and β-agglutinins, can pass through the placental barrier and cause hemolysis of fetal red blood cells. The conflict on the basis of inconsistency according to the AB0 system occurs in 10% of cases and proceeds, as a rule, benignly. It should be noted that the discrepancy between the blood of the fetus and the mother does not always lead to the development of the disease. For example, Rh incompatibility occurs in 5-10% of pregnancies, and Rh conflict - in 0.8%.
Pathogenesis in edematous form of hemolytic disease of the newborn
The edematous form, or dropsy of the fetus, occurs if hemolysis begins even in utero, from about 18-22 weeks of pregnancy, is intense and leads to the development of severe fetal anemia. As a result, severe fetal hypoxia occurs, which causes profound metabolic disorders and damage. vascular wall. An increase in the permeability of the vascular wall leads to the fact that albumin and water move from the fetal blood into the interstitium of tissues. At the same time, the synthesis of albumin in the baby's liver decreases, which aggravates hypoproteinemia.
As a result, a general edematous syndrome is still formed in utero, ascites develops, fluid accumulates in the pleural cavities, in the pericardial cavity, etc. A decrease in the drainage function of the lymphatic system exacerbates the development of ascites and the accumulation of fluid in other body cavities. Hypoproteinemia, accumulation of fluid in the cavities, combined with damage to the vascular wall, lead to the development of heart failure.
As a result of erythroid metaplasia in the organs and severe fibrosis in the liver, hepato- and splenomegaly is formed. Ascites and hepatosplenomegaly cause high standing of the diaphragm, which leads to lung hypoplasia. The increased amount of indirect bilirubin formed during hemolysis is excreted from the blood and tissues of the fetus through the placenta into the mother's body, so there is no jaundice at birth.
Pathogenesis in icteric form of hemolytic disease of the newborn
The icteric form of the disease develops if hemolysis begins shortly before childbirth. As a result of the destruction of red blood cells, the concentration of indirect (non-conjugated) bilirubin rapidly and significantly increases, which leads to the following changes:
- accumulation of indirect bilirubin in the lipid substances of tissues, which causes icteric staining of the skin and sclera - jaundice, as well as as a result of the accumulation of indirect bilirubin in the nuclei of the base of the brain, which leads to its damage with the development of neuronal necrosis, gliosis and the formation of bilirubin encephalopathy (nuclear jaundice);
- an increase in the load on liver glucuronyl transferase, which leads to the depletion of this enzyme, the synthesis of which begins in the liver cells only after birth, and as a result, hyperbilirubinemia is maintained and enhanced;
- increased excretion of conjugated (direct) bilirubin, which can lead to impaired bile excretion and the development of complications - cholestasis.
As with the edematous form, hepatosplenomegaly develops.
Pathogenesis of the anemic form of hemolytic disease
The anemic form develops when small amounts of maternal antibodies enter the fetal circulation shortly before delivery. At the same time, hemolysis is not intense, and the newborn's liver actively removes indirect bilirubin. Anemia dominates, and jaundice is absent or minimally expressed. Characterized by hepatosplenomegaly.
Symptoms of hemolytic disease of the newborn
Hemolytic disease of the newborn and fetus has three clinical forms: anemic, icteric and edematous. Among them, the most severe and prognostically unfavorable is edematous.
Common clinical signs of all forms of hemolytic disease of the newborn: pallor of the skin and visible mucous membranes as a result of anemia, hepatosplenomegaly. Along with this, edematous, icteric and anemic forms have their own characteristics.
edematous form
The most severe form of hemolytic disease of the newborn. The clinical picture, in addition to the above symptoms, is characterized by a common edematous syndrome: anasarca, ascites, hydropericardium, etc. Perhaps the appearance of hemorrhages on the skin, the development of DIC as a result of hypoxia, hemodynamic disorders with cardiopulmonary insufficiency. They note the expansion of the boundaries of the heart, the muffledness of its tones. Often after birth, respiratory disorders develop against the background of pulmonary hypoplasia.
Icteric form of hemolytic disease
This is the most common form of hemolytic disease of the newborn. In addition to general clinical manifestations, which include pallor of the skin and visible mucous membranes, as a rule, very moderate and moderate enlargement of the spleen and liver, jaundice is also noted, predominantly of a warm yellow hue. At the birth of a child, amniotic fluid, umbilical cord membranes, and primordial lubrication can be stained.
Characteristically early development jaundice: it occurs either at birth or in the first 24-36 hours of a newborn's life.
According to the severity of jaundice, there are three degrees of icteric form of hemolytic disease of the newborn:
- mild: jaundice appears by the end of the first or the beginning of the second day of a child's life, the content of bilirubin in the cord blood does not exceed 51 µmol/l, the hourly increase in bilirubin is up to 4-5 µmol/l, the liver and spleen are moderately enlarged - less than 2.5 and 1.0 cm respectively;
- moderate: jaundice occurs immediately at birth or in the first hours after birth, the amount of bilirubin in cord blood exceeds 68 µmol/l, the hourly increase in bilirubin is up to 6-10 µmol/l, liver enlargement is up to 2.5-3.0 cm spleen up to 1.0-1.5 cm;
- severe: diagnosed according to ultrasound of the placenta, indicators of the optical density of amniotic fluid bilirubin obtained during amniocentesis, the amount of hemoglobin and the hematocrit value of the blood obtained during cordocentesis. With delayed or inadequate treatment, the icteric form may be accompanied by the development of the following complications.
Nuclear jaundice
At the same time, symptoms indicating damage to the nervous system are noted. First, in the form of bilirubin intoxication (lethargy, pathological yawning, loss of appetite, regurgitation, muscle hypotension, disappearance of the II phase of the Moro reflex), and then bilirubin encephalopathy (forced body position with opisthotonus, "brain" cry, bulging of the large fontanelle, disappearance of the Moro reflex , convulsions, pathological oculomotor symptoms - a symptom of the "setting sun", nystagmus, etc.).
Bile thickening syndrome, when jaundice acquires a greenish tint, the liver is slightly enlarged compared to the previous days, there is a tendency to acholia, the saturation of urine color increases.
Anemic form of hemolytic disease of the newborn
The least common and most mild form of the disease. Against the background of pallor of the skin, lethargy, poor sucking, tachycardia, hepatosplenomegaly are noted, muffled heart sounds and systolic murmur are possible.
Along with changes in the body of the fetus, there are changes in the placenta. This is expressed in an increase in its mass. If normally the ratio of the mass of the placenta to the mass of the fetus is 1: 6, then with the Rhesus conflict it is 1: 3. The increase in the placenta occurs mainly due to its edema.
But this is not limited to pathology in Rh-conflict. In addition to the above, with Rhesus conflict, antenatal (prenatal) fetal death and repeated spontaneous abortions are noted.
Moreover, with a high activity of antibodies, spontaneous abortions can occur in the early stages of pregnancy.
In women who have had a Rhesus conflict, toxicosis of pregnancy, anemia, and liver function are more likely to develop.
Classification
Depending on the type of conflict, hemolytic disease of the newborn is distinguished:
- with incompatibility of erythrocytes of the mother and fetus according to the Rh factor;
- in case of incompatibility according to the ABO system (group incompatibility);
- with incompatibility for rare blood factors.
By clinical manifestations allocate:
- edematous form (anemia with dropsy);
- icteric form (anemia with jaundice);
- anemic form (anemia without jaundice and dropsy).
According to the severity, the icteric form is classified as mild, moderate and severe.
In addition, there are complicated (nuclear jaundice, bile thickening syndrome, hemorrhagic syndrome, damage to the kidneys, adrenal glands, etc.) and uncomplicated forms of hemolytic disease of the newborn.
Diagnosis of hemolytic disease of the newborn
Diagnosis of hemolytic disease of the newborn is based on an immunological examination of a pregnant woman, ultrasound, Doppler fetoplacental and uteroplacental blood flow, electrophysiological examination methods, amniotic fluid examination (during amniocentesis), cordocentesis and fetal blood test.
An immunological study allows you to determine the presence of antibodies, as well as a change in their number (increase or decrease in titer). Ultrasound allows you to measure the volume of the placenta, determine the increase in its thickness, detect polyhydramnios, an increase in the size of the liver and spleen of the fetus, an increase in the size of the fetal abdomen compared to the size of the head and chest, ascites in the fetus. Dopplerometry allows you to detect an increase in the systolic-diastolic ratio and resistance index in the umbilical artery and an increase in blood flow velocity in the fetal middle cerebral artery. Electrophysiological methods (cardiotocography with the determination of the fetal condition indicator) make it possible to detect a monotonous rhythm in moderate and severe forms of the disease and a "sinusoidal" rhythm in the edematous form of GBP. The study of amniotic fluid (during amniocentesis) allows you to determine the increase in the optical density of bilirubin in the amniotic fluid. Finally, cordocentesis and a study of the fetal blood can detect a decrease in hematocrit, a decrease in hemoglobin, an increase in the concentration of bilirubin, an indirect Coombs test and determine the fetal blood group, the presence of the Rh factor.
Since the prognosis for the disease depends on the content of bilirubin, then in a born child with suspected hemolytic disease of the newborn, in order to develop further medical tactics, it is first necessary to do biochemical analysis blood with the determination of the concentration of bilirubin (total, indirect, direct), protein, albumin, ACT, ALT, and then conduct an examination to determine the etiology of hyperbilirubinemia. For this purpose, the newborn is given general analysis blood, determine the Rh-affiliation with possible Rh-sensitization and the blood group with possible ABO-sensitization, determine the antibody titer and direct Coombs reaction.
Differential Diagnosis
Differential diagnosis of hemolytic disease of the newborn is carried out with other anemias. These include hereditary anemia due to the following disorders:
- violation of the morphology of erythrocytes (microspherocytosis, elliptocytosis, stomatocytosis);
- deficiency of erythrocyte enzymes (glucose-6-phosphate dehydrogenase, glutathione reductase, glutathione peroxidase, pyruvate kinase);
- anomaly in hemoglobin synthesis (a-thalassemia).
To exclude these diseases, you should carefully collect an anamnesis about the presence of other carriers of this pathology in the family and conduct the following studies:
- determination of erythrocyte morphology;
- determination of osmotic stability and diameter of erythrocytes;
- determination of the activity of erythrocyte enzymes;
- determination of the type of hemoglobin.
Treatment of hemolytic disease of the newborn
First of all, if we are talking about the Rh conflict, it is necessary to diagnose the disease even during the period of intrauterine development of the fetus, assess its severity and, accordingly, the prognosis of the disease, and treat it until the fetus reaches viability. All therapeutic and prophylactic methods used during this period of fetal life are divided into non-invasive and invasive.
Non-invasive methods
Non-invasive methods include plasmapheresis and the introduction of pregnant intravenous immunoglobulin.
Plasmapheresis of a pregnant woman is carried out for the purpose of detoxification, rheocorrection and immunocorrection.
Contraindications for plasmapheresis:
- severe damage to the cardiovascular system;
- anemia (hemoglobin less than 100 g/l);
- hypoproteinemia (less than 55 g/l);
- hypocoagulation;
- immunodeficiency state;
- history of allergic reactions to protein and colloid preparations, anticoagulants.
Immunoglobulin for intravenous administration is used to inhibit the production of own maternal antibodies and blockade of Rh-related antibodies during their placental transport. Immunoglobulin is used for intravenous administration at a dose of 0.4 g per kilogram of body weight of a pregnant woman. This dose is distributed over 4-5 days. It is necessary to repeat the courses of administration every 3 weeks until delivery. This method treatment is not considered universally recognized, since the outcome for the fetus improves slightly in severe cases of the disease.
Invasive methods
Invasive methods include cordocentesis and intrauterine transfusion of red blood cells. These procedures are carried out only with Rh-sensitization, currently this is the only pathogenetic method for the treatment of hemolytic disease of the fetus.
Indications for cordocentesis:
- aggravated obstetric history (death of previous children from severe forms of hemolytic disease of the newborn);
- high antibody titer (1:32 and above);
- with ultrasound - signs of hemolytic disease of the fetus;
- high values of the optical density of bilirubin in amniotic fluid obtained during amniocentesis (3rd zone of the Lily scale).
The terms during which cordocentesis is performed: from the 24th to the 35th week of pregnancy.
An indication for intrauterine transfusion of erythrocyte mass if a positive test is found in the fetus Rh factor is a decrease in hemoglobin and hematocrit by more than 15% of the norm, determined at a given gestational age. For intrauterine transfusion of erythrocyte mass, only "washed" erythrocytes of the 0 (1) blood group Rh-negative are used. Intrauterine transfusion of erythrocyte mass is carried out according to indications 1-3 times.
Treatment of hemolytic disease of the newborn, in contrast to the treatment of hemolytic disease of the fetus, includes, first of all, the treatment of hyperbilirubinemia, secondly, the correction of anemia, and, finally, post-syndromic therapy aimed at restoring the functions of various organs and systems. All newborns with this disease are not applied to the breast, but are fed artificially in the first 5-7 days of life, since antibodies can penetrate with a woman's breast milk and be absorbed in the intestines of newborns, which leads to increased hemolysis.
Treatment of hyperbilirubinemia
Treatment of hyperbilirubinemia involves the use of conservative and surgical therapy. Start with conservative treatment, and at critical values of bilirubin, they are combined with operational - exchange (exchange) blood transfusion (ZPK).
Conservative therapy includes phototherapy (PT) and intravenous immunoglobulin. Infusion therapy, on the recommendation of the Russian Association of Perinatal Medicine Specialists (RASPM), is carried out in cases where it is impossible to adequately feed the child. Phenobarbital is currently practically not used due to the fact that the onset of the effect is significantly delayed from the moment it was started, and against the background of use, the syndrome of CNS depression intensifies.
Phototherapy
The mechanism of action of phototherapy is based on the fact that when it is carried out on irradiated areas in the skin and subcutaneous fat layer at a depth of 2-3 mm, as a result of the processes of photooxidation and photoisomerization, a water-soluble isomer of indirect bilirubin, lumirubin, is formed, which then enters the bloodstream and is excreted with bile and urine.
Indications for phototherapy:
- yellowness of the skin at birth;
- high concentration of indirect bilirubin.
Principles of phototherapy:
- radiation dose - not less than 8 μW/(cm2xnm);
- observe the distance from the source to the patient, specified in the instructions for the device;
- the child should be placed in the incubator;
- the eyes and genitals of the child should be protected;
- the position of the child under the FT lamps should be changed every 6 hours.
Minimum indirect bilirubin concentrations (µmol/l) at which phototherapy is indicated
Phototherapy is carried out continuously with breaks for feeding the child for 3-5 days. FT should be canceled when the content of indirect bilirubin drops below 170 µmol/L.
During phototherapy, various reactions and side effects can occur.
Complications and side effects of phototherapy
|
Manifestations |
Development mechanism |
Events |
|
Syndrome of "tanned skin" |
Induction of melanin synthesis |
Observation |
|
Bronze Child Syndrome |
Accumulation of direct bilirubin photooxidation products |
Cancel FT |
|
Activation of the secretory function of the intestine |
Observation |
|
|
lactase deficiency |
Serous lesions of the villous epithelium |
|
|
Damage to circulating red blood cells as a result of photosensitivity |
Cancellation of FT |
|
|
Skin burns |
Excessive lamp emission |
Cancellation of FT |
|
Increased fluid loss |
Increase your child's fluid intake |
|
|
Skin rashes |
Increased formation and release of histamine during photosensitivity |
Observation, if necessary - cancellation of FT |
If signs of cholestasis appear, as evidenced by an increase in the fraction of direct bilirubin by 20-30% or more, an increase in the activity of ACT and ALT, alkaline phosphatase, cholesterol concentration, the time of phototherapy should be limited to 6-12 hours / day or completely canceled in order to avoid development syndrome "bronze child".
Use of immunoglobulin
Immunoglobulin for intravenous administration is used to block Fc receptors, which prevents hemolysis. An early start of the introduction of immunoglobulin (in the first 2 hours of life) is necessary, which is possible only with antenatal diagnosis of the disease. Later introduction of immunoglobulin is possible, but less effective.
Standard immunoglobulins for intravenous administration are used: sandoglobin, ISIVEN (Italy), polyglobin Np (Germany), etc.
Possible schemes for the administration of immunoglobulins:
- 1 g/kg every 4 hours;
- 500 mg/kg every 2 hours;
- 800 mg/kg daily for 3 days.
Regardless of the dose and frequency, a proven (95%) positive effect was obtained, which manifested itself in a significant decrease in the incidence of PKD and the duration of phototherapy.
Infusion therapy
Infusion therapy is carried out in cases where it is not possible to adequately drink the child against the background of ongoing phototherapy. The daily volume of liquid administered to the child must be increased by 10-20% (in children with extremely low body weight - by 40%) compared with the physiological need.
When carrying out infusion therapy, one should monitor the child's body weight, evaluate diuresis, electrolytes, blood glucose, and hematocrit.
Fluid therapy mainly involves transfusion of 10% glucose solution4. Infusion therapy is carried out intravenously or intragastrically through a gastric tube. Intragastric fluid administration can be started from the 3-4th day of life, to prevent the development of cholestasis, a 25% solution of magnesium sulfate can be added to the dropper at the rate of 5 ml / kg, no-shpa - 0.5 ml / kg, 4% potassium solution chloride - 5 ml/kg. With intragastric fluid administration, there is no need to reduce the amount of feeding.
Operative Therapy - Exchange Transfusion
Distinguish between early (in the first 2 days of life) and later (from 3 days of life) PPC.
The indication for late PKC is the concentration of indirect bilirubin, equal to 308-340 µmol / l (for a full-term newborn).
Indications for late exchange transfusion in newborns depending on birth weight
1 * Minimum values of bilirubin - an indication for the start of appropriate treatment in cases where the child's body is affected by pathological factors that increase the risk of bilirubin encephalopathy (anemia; Apgar score at the 5th minute less than 4 points; Pa02 less than 40 mm Hg. longer than 1 hour, pH arterial blood less than 7.15 lasting more than 1 hour; rectal temperature less than 35 °C; albumin concentration less than 25 g/l; deterioration of the neurological status against the background of hyperbilirubinemia; generalized infectious disease or meningitis).
When the first symptoms of bilirubin intoxication appear, immediate PKK is indicated, regardless of the concentration of bilirubin.
Choice of drugs for exchange transfusion
In isolated Rh-conflict, a Rh-negative erythrocyte mass and plasma of the same group as the child's blood is used, but it is possible to use plasma of the AB (IV) blood group. In case of an isolated group conflict, the erythrocyte mass of the 0(1) group is used, which matches the Rh factor with the Rh factor of the child's erythrocytes, and AB(IV) plasma or one group with the child's blood group. If it is possible to develop both Rh-incompatibility and incompatibility according to the ABO system, as well as after intrauterine blood transfusions, Rh-negative erythrocyte mass of 0 (1) blood group and AB (IV) plasma or one group with the child's blood group are used for PPC.
In hemolytic disease of a newborn with a conflict on rare blood factors, donor blood is used that does not have a "conflict" factor.
Calculation of the volume of drugs for exchange transfusion
The total volume is 1.5-2 BCC, i.e. for a full-term baby, about 150 ml / kg, and for a premature baby, about 180 ml / kg.
The ratio of erythrocyte mass and plasma depends on the initial concentration of hemoglobin before the start of the operation. The total volume consists of the volume of packed cells needed to correct the anemia and the volume of packed cells and plasma needed to achieve the PPC volume. The volume of erythrocyte mass required to correct anemia is calculated by the formula:
the volume of red blood cells (ml) \u003d (160 - the hemoglobin of the child in g / l) x 0.4 x the weight of the child in kg.
From the total volume, the volume of red blood cells needed to correct anemia should be subtracted; the remaining volume is replenished with erythrocyte mass and plasma in a ratio of 2:1. The above approximately corresponds to the following ratio of erythrocyte mass, depending on the concentration of hemoglobin in the child.], , ,
Exchange transfusion technique
ZPK is carried out through one of the large vessels (umbilical vein, subclavian vein). Before the PPC, blood is taken to determine the concentration of bilirubin, the compatibility of the blood of the donor and the recipient. ZPK is carried out by the "pendulum method", i.e. withdrawing and introducing alternately a portion of blood at the rate of up to 5-7 ml per kilogram of the child's weight. Before the start of the PKK, plasma can be administered at a rate of 5 ml/kg. ZPK begins with the removal of blood. Prior to the start of the PKC and throughout it, the catheter is washed with sodium heparin solution.
When the initial concentration of hemoglobin is below 80 g/l, FPC begins with the correction of anemia, i.e. with the introduction of only erythrocyte mass under the control of hemoglobin content. After reaching a hemoglobin concentration of 160 g/l, erythrocyte mass and plasma are injected. To do this, you can dilute the erythrocyte mass with plasma, or you can alternately inject two syringes of the erythrocyte mass and one plasma syringe.
At the end of the ZPK, blood is taken again to determine the concentration of bilirubin. After PKK, conservative therapy is continued.
ZPK can be accompanied by the development of immediate and delayed side effects.
Complications of exchange transfusion
|
Manifestations |
Events |
|
|
cardiac |
Cardiac control |
|
|
Volume overload |
||
|
Heart failure |
||
|
Vascular |
Thromboembolism, air embolism |
Compliance with blood transfusion technique |
|
Flushing the catheter with sodium heparin solution |
||
|
Coagulation |
Overdose of heparin sodium |
Dose control of heparin sodium |
|
Thrombocytopenia |
Platelet count control |
|
|
electrolyte |
Hyperkalemia |
For prevention, for every 100 ml transfused (erythrocyte mass and plasma in total), inject 1-2 ml of a 10% calcium gluconate solution |
|
hypocalcemia |
||
|
Hypernatremia |
Control |
|
|
KOS control |
||
|
infectious |
Viral |
Donor control |
|
Bacterial |
Antibacterial therapy is prescribed to prevent complications after PPC and for the time the catheter is in a large vessel. |
|
|
Mechanical destruction of donor cells |
Control |
|
|
Necrotizing enterocolitis |
Observation, detection of clinical symptoms, appropriate therapy |
|
|
Hypothermia |
Body temperature control, warming |
|
|
hypoglycemia |
For prophylaxis, for every 100 ml transfused (erythrocyte mass and plasma in total), inject 2 ml of 10% glucose solution4 |
|
|
Graft-versus-host reaction |
Transfuse irradiated blood products |
|
|
Do not use large volumes for FPC |
||
Late anemia develops 2-3 weeks after PKD. It usually has a hyporegenerative and hypoerythropoietic character. For its correction, recombinant erythropoietin is used (epoetin alfa subcutaneously 200 IU/kg once every three days for 4-6 weeks).
If iron deficiency is detected during treatment with recombinant erythropoietin, iron preparations are included in therapy at a dose of utilizable iron of 2 mg/kg orally.
Prevention
Prevention is designed for women with Rh-negative blood. There is no prevention of group incompatibility.
To prevent the development of Rh-sensitization, all women with Rh-negative blood should enter one dose of anti-D-rhesus immunoglobulin.
To prevent all the negative consequences of the Rh conflict and the conflict on other blood factors, it is necessary to determine the blood type of the future mother and, if it turns out that there is Rh-negative blood, then you should find out if this woman has received Rh-positive blood (and in general, whether any blood was transfused); find out what the real pregnancy is (whether there were earlier artificial or spontaneous abortions, intrauterine death of the fetus, premature birth or death of the newborn shortly after birth from jaundice). Importance also has information about the Rh-affiliation of the father of the unborn child.
For the purpose of prevention, in addition to all of the above, anti-Rhesus - immunoglobulin is used. This is done either after the birth of an Rh-positive child, or after the first induced abortion. It is administered to the puerperal intramuscularly, once, no later than 72 hours after childbirth. This specific prevention of the Rh conflict is possible only in non-sensitized women (sensitization - increased sensitivity), that is, those who have not received Rh-positive blood transfusions, they have not had abortions or miscarriages, and, in general, this pregnancy is the first.
In addition to specific prophylaxis, non-specific prophylaxis is also carried out. It includes various medications that reduce the sensitization of the body and increase its immunobiological defenses. Sometimes, for the same purpose, transplantation of a pregnant skin flap of her husband is used.
], [HDN- a pathological condition resulting from the incompatibility of the blood of the mother and fetus for some antigens, in which hemolysis of fetal erythrocytes occurs under the influence of maternal isoantibodies penetrating the placental barrier.
Etiology and pathogenesis. The conflict most often develops according to erythrocyte antigens Rh-Hr and AB0.
Reasons for isoimmunization:
a) iatrogenic - associated with the introduction of Rh-positive blood into a woman's body when she underwent blood transfusions in the past or during autohemotherapy;
b) fetal-maternal transplacental transfer of fetal erythrocytes into the mother's bloodstream during pregnancy and childbirth.
When the antigen first enters the mother's bloodstream, class M immunoglobulins are produced, the molecules of which are of considerable size and do not penetrate the placental barrier to the fetus. The entry of the antigen into the mother's bloodstream during repeated pregnancy causes a rapid secondary immune response in the form of the formation of small class G immunoglobulins, which, freely penetrating the placental barrier, are deposited on the membrane of the erythrocytes of the Rh-positive fetus, leading to their hemolysis and accelerated destruction in the organs. reticuloendothelial system. Massive destruction of red blood cells leads to the development of anemia in the fetus, the appearance of which causes an increase in the concentration of erythropoietin in the bloodstream of the fetus. Erythropoietin stimulates hematopoiesis, as a result of which foci of extramedullary hematopoiesis appear, mainly in the liver and spleen of the fetus, which increase significantly. Extramedullary hematopoiesis is characterized by incomplete development of erythrocytes and the appearance of erythroblasts in the circulation.
clinical picture. Allocate anemic, icteric and edematous form of the disease.
1. anemic form. Manifested from the first hours of life. The main symptoms are pale skin, low level hemoglobin and erythrocytes, petechial rashes, physical inactivity, enlargement of the liver and spleen. Anemia develops not so much due to hemolysis, but as a result of inhibition of bone marrow function and a delay in the release of immature and mature forms of erythrocytes from it.
2. icteric form. The most important symptoms are jaundice, anemia, enlargement of the liver and spleen. In severe cases, symptoms of CNS damage are observed. At the birth of a child, icteric staining of amniotic fluid, original lubricant, and skin is often noticed. Anemia is more often normochromic or hyperchromic and usually does not reach a pronounced degree. The appearance and intensification of jaundice are due to an increase in the level of indirect bilirubin in the blood. As jaundice increases, the child's condition worsens, symptoms appear that indicate CNS damage: convulsive twitches, nystagmus, hypertonicity, etc. Symptoms of "nuclear jaundice" develop (with bilirubin equal to 307.8 - 342.0 μmol / l).
3. edematous form. Pronounced symptoms of the disease are general edema (anasarca, ascites), large liver and spleen, significant anemia, less pronounced jaundice (due to a large amount of fluid in the body), hemodynamic disorders (hypervolemia, increased venous pressure, stagnation in the pulmonary circulation, cardio - pulmonary insufficiency). Hemorrhagic syndrome is often observed.
TTH according to the ABO system, as a rule, does not have specific manifestations at the time of the birth of the child.
The severity of HDN according to the Rh factor:
a) mild form(I degree of severity) is characterized by some pallor of the skin, a slight decrease in the concentration of hemoglobin (up to 150 g / l) and a moderate increase in the level of bilirubin in the cord blood (up to 85.5 μmol / l), slight pastiness of the subcutaneous fatty tissue;
b) moderate form (II degree of severity) is characterized by pallor of the skin, a decrease in the level of hemoglobin (150 - PO g / l), an increase in the content of bilirubin in the cord blood (85.6 - 136.8 μmol / l), pasty subcutaneous tissue, enlargement of the liver and spleen;
c) severe form (III degree of severity) is characterized by a sharp pallor of the skin, a significant decrease in hemoglobin levels (less than 110 g / l), a significant increase in the content of bilirubin in the cord blood (136.9 μmol / l or more), generalized edema.
The most severe complication of HDN is bilirubin encephalopathy- is associated with toxic damage to neurons by indirect bilirubin.
Factors that increase the risk of CNS damage: prematurity, asphyxia, hypothermia, acidosis, hypoproteinemia, malnutrition.
There are 4 phases of the course of bilirubial encephalopathy:
1) bilirubin intoxication - lethargy, hypo-, adynamia, hypo-, areflexia;
2) signs of nuclear jaundice - spasticity, convulsions, "brain scream", a symptom of the "setting sun";
3) imaginary well-being - from the 2nd week, a decrease in spasticity, seizures;
4) the formation of a clinical picture of neurological complications - children cerebral paralysis, athetosis, paralysis, paresis, deafness.
Diagnostics.
1. Immunological analysis - detection of Rh-sensitized women.
2. CTG, ultrasound - detection of signs of chronic hypoxia.
3. Study of amniotic fluid.
4. Immediately after the birth of a child from a woman with a Rh-negative blood type, the child's blood type, hemoglobin and bilirubin levels are determined, and a Coombs test is performed.
Treatment.
1. Non-specific desensitization of all pregnant women with Rh "-" blood. It is carried out for 10-12 days with a period of 10-12, 22-24, 32-34 weeks. Intravenous administration of 20 ml of 40% glucose with 2 ml of 5% ascorbic acid solution, 2 ml of 1% sigetin and 100 mg of cocarboxylase is used. Inside prescribe rutin, teonikol, calcium gluconate, iron preparations, tocopherol, antihistamines.
2. Transplantation of the husband's skin flap to pregnant women.
3. With severe sensitization in complex therapy include prednisolone 5 mg daily from 28 weeks of gestation.
4. Plasmapheresis and hemosorption are performed for pregnant women with a burdened history.
5. Children with a mild form of HDN are born in a satisfactory condition and do not need resuscitation. Their condition should be monitored dynamically. Such children should start phototherapy from the first hours of life.
6. Children with a moderate form of HDN according to the Rh factor can be born in a state of asphyxia. After providing the necessary resuscitation measures, they should be transferred to the intensive care unit, where they urgently need to establish an adequate infusion of 10% glucose solution and phototherapy. Treatment is carried out under constant monitoring of the level of Hb, Ht in the peripheral blood, the level of bilirubin (every 6 hours on the 1st day).
With the ineffectiveness of conservative therapy, it is necessary to carry out a replacement blood transfusion.
7. Children with severe HVN require resuscitation in the delivery room. After completion of primary resuscitation, it is necessary to stabilize hemodynamics, perform umbilical vein catheterization, and perform partial PBV. To correct severe anemia in the edematous-anemic form of HDN, a partial replacement of the child's blood with an Rh-negative donor erythrocyte mass (without plasma injection) of group 0 (1) is immediately carried out at the rate of 60-70 ml/kg. At the end of the operation, the child should be given an infusion of fresh frozen plasma at a rate of 10-15 ml-kg and 10% glucose solution, at a constant rate. Depending on the severity of symptoms of respiratory and cardiovascular insufficiency, adequate post-syndromic therapy should be carried out.
Children with TTH for AB0 and rare blood factors require the same care and treatment as children with TTH for Rh.
Indications for ZPK:
1. Emergency FRA in severe HDN (using the partial FRA technique).
2. Early PPC (in the first 24 hours of life):
a) the level of total bilirubin in cord blood is above 77.5 µmol/l;
b) cord blood Hb level below 110 g/l; Ht below 35%;
c) an hourly increase in bilirubin above 8.5 μmol / l - rapidly progressive anemia (a drop in blood Hb levels below 120 g / l on the first day of life, even with a relatively low increase in bilirubin). In this case, the ZPK technique with the substitution of 2 BCC is used.
3. Later ZPK:
a) an increase in the concentration of total bilirubin in the blood serum of more than 256 µmol/l on the 2nd day of life and more than 340 µmol/l in full-term babies and more than 256-340 µmol/l in premature babies on the following day;
b) clinical signs of bilirubin intoxication serve as an indication for the conduction of PPC at any level of bilirubin. In this case, the ZPK technique with the substitution of 2 BCC is used.
ZPK operation technique:
1. Before starting the operation, hands are treated according to generally accepted methods, sterile gowns and gloves are put on.
2. ZPK is carried out through a sterile polyethylene inserted into the vein of the umbilical cord to a depth equal to the distance from the umbilical ring to the xiphoid process plus 1 cm upward towards the liver.
3. Before starting the procedure, it is necessary to flush the catheter with a weak solution of heparin: no more than 5-10 IU per 1 ml, i.e. 0.1 ml of the standard solution (5000 IU in 1 ml) should be diluted in 50 - 100 ml of sterile isotonic sodium chloride solution.
4. A catheter is inserted into the umbilical cord vein filled with isotonic sodium chloride solution or a weak solution of heparin, since during the child's cry, negative pressure may occur in the vein, and air may enter it from an empty catheter.
5. The first portions of blood obtained from the catheter are collected in several test tubes: to determine the blood group, bilirubin level and compatibility (for all, no more than 5-10 ml of the child's blood).
6. Fractional portions of 10-20 ml slowly remove the child's blood and replace it with the blood or erythrocyte mass of the donor in the same amount. In the latter case, for every 2 volumes of injected erythrocyte mass, 1 volume of plasma is administered.
7. After the introduction of every 100 ml of blood for the prevention of hypocalcemia, it is necessary to add 2 ml of 10% calcium gluconate solution or 2 ml of 10% calcium chloride solution, diluted with 2 ml of 10% glucose solution.
8. After replacing 2 BCC, the operation can be completed. The average duration of the operation is 1.5 - 2.5 hours. Faster and slower operation can adversely affect the general condition of the child.
9. The operation is completed intravenous administration broad spectrum antibiotic. The catheter is removed.
Complications in PKK: heart failure (with rapid administration, volume overload); cardiac arrhythmias (decrease in calcium and increase in potassium content); infection; thromboembolism; perforation of the umbilical vein and intestines; portal hypertension; anaphylactic shock; acute renal failure, hematuria; DIC syndrome (decrease in the number of platelets, deficiency of procoagulants); excessive heparinization; hypokalemia, acidosis, hyperkalemia, hypocalcemia; graft-versus-host reaction; hypothermia.
Low hemoglobin in newborns threatens with severe complications. A condition such as hemolytic disease of the newborn is encountered by the physician in about 0.6% of deliveries. At the same time, low hemoglobin in a premature baby is characteristic, rather than in a term-born baby. Manipulation such as replacement blood transfusion in newborns will help to cope with the condition.
Anemia in infants is said when hemoglobin at 1-2 weeks of life does not exceed 140 g / l, and erythrocytes 4.5 * 10 12 / l, while the hematocrit decreases by less than 40%. From 3-4 weeks of extrauterine development, the lower limit of the norm is 120 g / l and erythrocytes 4.0 * 10 12 / l.
The causes of anemia in a newborn are divided into three groups:
- Posthemorrhagic - as a result of blood loss due to rupture of the umbilical cord, pathology of the placenta, hemorrhages in the body cavity, cephalohematoma, bleeding from the intestines, etc.
- Hemolytic - the cause is the pathological destruction of red blood cells during immune processes, toxic effects, radiation. An example is hemolytic disease of the fetus and newborn with Rhesus conflict.
- Aplastic, hypoplastic or deficient - insufficiency of erythrocyte synthesis. An example is early anemia in preterm infants.
- Mixed form - an example is a decrease in hemoglobin in generalized infections. Includes iron deficiency, hemolytic, hypoplastic and other forms.
Early anemia of premature babies, RAS, develops in 1-2 months of the neonatal period. The main reason for this condition is the correspondence of high growth rates of body weight and BCC with the ability of erythropoiesis to reproduce new red blood cells. In preterm infants, erythropoietin production is significantly inferior to that of mature infants.
Anemia in premature babies weighing up to 1500 kg is often associated with phlebotomy losses - as a result of blood sampling for tests. The transfusion of erythrocyte mass with low hemoglobin in such babies in 15% of cases was provoked by blood sampling.
Hemolytic disease of the newborn
The reasons
Hemolytic disease of the newborn, or HDN, is a condition associated with the development of an immunological conflict between the blood of the mother and the fetus, when antigens are placed on the child's red blood cells, and antibodies to them are produced by the mother's body.

It is possible to notice hemolytic disease of the fetus and prevent its further development already at 18-24 weeks of gestation. In the first week of life, neonatal anemia is detected, in some cases, the hemoglobin level in an infant may decrease in the first months of life as a result of hemolysis of red blood cells in utero.
The basis for the development of an immunological conflict is the sensitization of a positive Rh factor antigen when it enters the mother's bloodstream. This can happen as a result of past pregnancies, especially those that ended in abortion or traumatic childbirth, preeclampsia, extragenital pathology in the mother.
During gestation, fetal erythrocytes normally enter the mother's body in scanty amounts - 0.1-0.2 ml, and during childbirth - 3-4 ml. But this is already enough for a primary immune response to occur and antibodies to develop. They belong to class M immunoglobulins, which are quite bulky to cross the placenta. Therefore, the child from the first pregnancy is not likely to face hemolytic disease of the newborn.
During the period of repeated gestation, class G immunoglobulin is produced, which easily penetrates the fetal bloodstream and causes hemolysis of its erythrocytes, the fetal hemoglobin level drops rapidly, and bilirubin increases.
Classification
There are several options for intrauterine incompatibility between mother and child:
- according to the Rh factor, when the mother is Rh-, and the fetus is Rh +;
- by group, if the mother is 0 (Ⅰ), the fetus has A (Ⅱ), B (Ⅲ) groups;
- rare cases when there is a conflict in the systems of Kell, Duffi, Kidd, etc.
According to the clinical symptoms, HDN is classified as follows:
- edematous form;
- icteric;
- anemic.
Hemolytic disease of the fetus GBP

The icteric form progresses shortly before delivery, hemolysis is so pronounced that a huge amount of indirect bilirubin accumulates in the blood. It is deposited in the nuclei of the brain, causing cerebral manifestations up to coma.
The anemic form is the safest, developing in response to the introduction of a small amount of antigen into the mother's bloodstream before childbirth. In addition to a decrease in hemoglobin, infants do not have complications.
Symptoms of HDN
At birth with HDN, there are symptoms according to the form of the disease. The edematous form is characterized by the following symptoms:
- massive edema from pastosity to anasarca;
- development of jaundice and low hemoglobin in infants;
- the liver and spleen are enlarged;
- severe hemorrhagic manifestations: impaired blood clotting;
- cardiopulmonary insufficiency;
- slight jaundice.
Icteric form:
- jaundice;
- hepatosplenomegaly;
- stagnation of bile;
- with an increase in the level of bilirubin, neurological symptoms occur;
- development of bilirubin encephalopathy - stage 1 reversible with lethargy, impaired sucking, apnea, stage 2 - opisthotonus, neck stiffness, convulsions, stages 3 and 4 with progressive deterioration.
Anemic form:
- pallor of the skin and mucous membranes;
- hemoglobin is lowered in infants up to 2 months;
- lethargy and adynamism;
- tachycardia;
- hepatosplenomegaly.
The disease is more severe in premature babies.
Replacement (exchange) blood transfusion in newborns
Indications

Hemolytic disease of the newborn can lead to severe complications and even death of the child. This life-threatening condition can be eliminated by replacement, or exchange, blood transfusion to a newborn instead of his own, hemolyzed blood.
The indications for the operation of the exchange transfusion of blood ZPK according to Diamond are:
- treatment of edematous form of HDN;
- ineffective phototherapy for icteric.
Allocate early ZPK and later. The first is carried out at 2 days from birth, and the second - from the third day.
Laboratory data indicating the need for early exchange transfusion are for full-term newborns:
- bilirubin from the umbilical cord - 68 µmol / l;
- hourly increase in bilirubin more than 9 µmol/l.
The requirements for starting an exchange transfusion with low hemoglobin in premature babies are tougher - hourly increase in bilirubin should be no more than 8 µmol/l. This is due to the failure of the enzymatic system of the premature.
Late replacement blood transfusion (from the third day) is indicated in term infants when bilirubin is greater than or equal to 342 µmol/L. In premature babies, however, they resort to late PPC, depending on birth weight and age. Below is a table of this relationship.
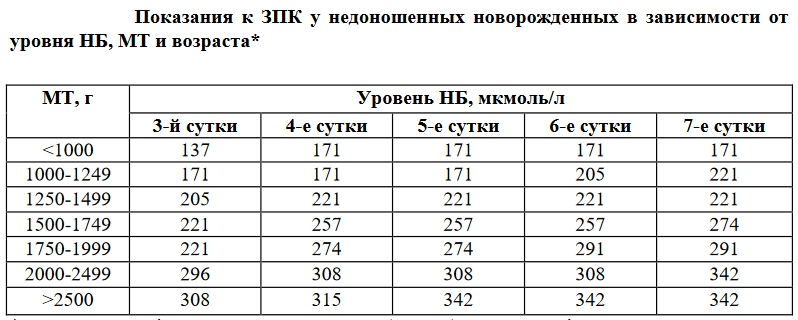
It is important to know that an exchange transfusion operation can be performed even earlier, when indirect bilirubin has not reached its critical values. This is possible if there are predictors of bilirubin encephalopathy:
- at the 5th minute after birth, according to Apgar, the child is estimated at less than 3 points;
- total protein below 50 g/l, and albumin - 25 g/l;
- glucose< 2,2 ммоль/л;
- the fact of generalization of infection or meningitis;
- partial pressure of carbon dioxide on exhalation up to 40 mm Hg for more than 1 hour;
- arterial blood pH less than 7.15 for more than 1 hour;
- rectal temperature is equal to or less than 35 degrees;
- exacerbation of neurological symptoms in hyperbilirubinemia.
What is transfused
If there is a severe hemolytic disease of the newborn, then the method of partial operation of the ZPK is immediately used, when erythrocytes of the first group of a negative Rh factor are injected before determining the group and Rh in the child. Dose - 45 ml / kg.
If the baby has incompatibility only for the Rh factor, then he is transfused with an Rh-negative erythrocyte mass or washed erythrocytes of his own group and fresh frozen plasma, and Ⅳ of the group is possible. Do not use Rh-positive red blood cells.
During the PKK operation, use only freshly prepared erythrocytes - no later than 72 hours from the collection.
If there is a conflict in the blood type, then use the red blood cell mass or washed red blood cells of the first 0 (Ⅰ) group, with Rh as in the child's red blood cells, AB plasma (Ⅳ) or the child's blood group. It is impossible to transfuse erythrocytes of the same group as the baby.
If there is a combination of incompatibility for the group and the Rh factor, and also when PKK was performed in utero, then the erythrocyte mass 0 (Ⅰ) of the Rh-negative group and AB plasma (Ⅳ) or the same group as the child are infused.
If there is incompatibility due to rare factors, then donor erythrocytes that do not have an antigen are used for transfusion.

How to choose a dose
The total volume of the medium for administration should be 2 volumes of the circulating blood of a newborn, and this is 160-180 ml / kg - full-term, 180 ml / kg - premature babies. The ratio of mass to plasma in this volume will be determined by the initial level of hemoglobin. The total PZK volume includes the RBCs required to correct anemia in the newborn + the RBC mass and plasma required to achieve the PZK volume.
Er. weight in ml = (160 - Hb (g / l) actual) x 0.4 x weight of the child (kg).
The resulting figure must be subtracted from the total volume for the ZPK. After that, the remaining volume is replenished with erythrocyte mass and plasma in a ratio of 2:1.
Preparing for the ZPK
Before performing an exchange transfusion operation, the following conditions must be met:
- eliminate acidosis, hypoxemia, hypoglycemia, hypotension, hypothermia;
- prepare a flask with a source of radiant light;
- exclude enteral nutrition 3 hours before the procedure;
- setting a gastric tube for periodic removal of contents;
- perform a cleansing enema;
- preparation of instruments: umbilical catheters, syringes of various sizes, etc.;
- warming the transfusion medium;
- organize everything necessary for resuscitation;
- the donor's blood must be checked for group affiliation and compatibility with the recipient's serum;
- before performing the procedure, observe asepsis, cover the manipulation area with sterile wipes, treat the doctor's hands and the area of operation.
Methodology

After the preparatory stage, the doctor and assistant perform such manipulations of the replacement (exchange) blood transfusion.
- After cutting off the top of the umbilical cord residue, a sterile catheter is inserted 3-5 cm (in large children 6-8 cm) towards the liver. In case of late blood transfusion after 4 days from birth or with existing contraindications for placing an umbilical catheter, transfusion is performed through another accessible central vein.
- The catheter is filled with a heparinized solution of 0.5-1 U/ml.
- The child's blood is withdrawn (taken) by 10-20 ml, and in premature babies by 5-10 ml.
- Enter the erythrocyte mass and plasma in the equivalent of the taken. After 2 syringes of er.mass, 1 syringe of plasma follows.
- After replacing 100 ml of the volume of the required infusion, 1-2 ml of calcium gluconate solution or 0.5 ml of calcium chloride solution in 5-10 ml of 10% glucose solution should be injected.
- Complete the operation after replacing 2 volumes of circulating blood. The duration of the procedure should be 1.5-2.5 hours.
- Before completion, you need to take blood to evaluate bilirubin.
- Before removing the catheter, inject half the daily dose of antibiotic.
- After completing the procedure, apply a sterile dressing to the wound.
The effectiveness of the exchange transfusion operation is evidenced by a more than twofold drop in the concentration of bilirubin by the end of the manipulation.
In the postoperative period, mandatory monitoring of glycemia, calcium, potassium, acidity, hemodynamics, and infection is necessary. Further treatment includes phototherapy. If late anemia is formed, erythropoietin preparations are prescribed - Epoetin alfa.
Complications
The most severe complications develop immediately after OZPK:
- arrhythmia;
- cessation of the work of the heart;
- thrombosis;
- hyperkalemia;
- thrombocytopenia;
- the occurrence of an infection;
- hypocalcemia;
- acidosis;
- hypothermia;
- necrotizing enterocolitis.
Conclusion
The edematous form is the most unfavorable for the prognosis - children often die with it. Icteric - successfully treated with timely replacement (exchange) blood transfusion, if there is no damage to the central nervous system. The most favorable anemic form in terms of survival. Mortality in HDN is 2.5%, the majority is edematous.



