Description of the cardiogram of the heart. Deciphering electrocardiography: norm and pathology
The term "EKG" stands for "electrocardiogram". This is a graphical recording of the electrical impulses of the heart.
The human heart has its own pacemaker. The pacemaker is located directly in the right atrium. This place is called the sinus node. The impulse that comes from this node is called a sinus impulse (it will help to decipher what the ECG will show). It is this source of impulses that is located in the very heart and itself generates electrical impulses. Then they are sent to the conducting system. Impulses in people who do not have cardiac pathology pass evenly through the conductive cardiac system. All these outgoing impulses are recorded and displayed on the cardiogram tape.
From this it follows that an ECG - an electrocardiogram - is a graphically registered impulses of the cardiac system. Will an EKG show heart problems? ? Of course it's great and fast way identify any heart disease. Moreover, the electrocardiogram is the most basic method in diagnosing the detection of pathology and various diseases hearts.
Created by the Englishman A. Waller back in the seventies of the XIX century. Over the next 150 years, the device that records the electrical activity of the heart has undergone changes and improvements. Although the principle of operation has not changed.
Modern ambulance teams are necessarily equipped with portable ECG devices, with which you can make an ECG very quickly, saving valuable time. With the help of an ECG, you can even diagnose a person. An ECG will show heart problems: from acute cardiac pathologies to In these cases, not a minute can be lost, and therefore a timely cardiogram can save a person's life.
Doctors of ambulance teams themselves decipher the ECG tape and, in case of acute pathology if the device shows a heart attack, then, including a siren, the patient is quickly taken to the clinic, where he will be immediately provided urgent help. But with problems, urgent hospitalization is not necessary, everything will depend on what the ECG shows.
When is an electrocardiogram prescribed?
If a person has the symptoms described below, then the cardiologist directs him to an electrocardiogram:
- swollen legs;
- fainting states;
- have shortness of breath;
- pain in the sternum, in the back, pain in the neck.
An ECG is necessarily assigned to pregnant women for examination, to people in preparation for surgery, medical examination.
Also ECG results are required in case of a trip to a sanatorium or if permission is needed for any sports activities.

For prevention and if a person has no complaints, doctors recommend taking an electrocardiogram once a year. Often this can help diagnose cardiac pathologies that are asymptomatic.
What will the ECG show
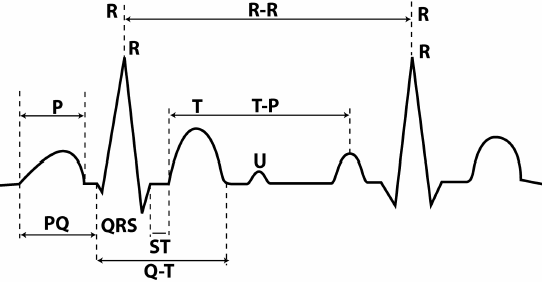
On the tape itself, the cardiogram can show a collection of prongs as well as recessions. These teeth are denoted by capital Latin letters P, Q, R, S and T. When deciphering, the cardiologist studies and deciphers the width, height of the teeth, their size and the intervals between them. These indicators can be used to determine general state heart muscles.
With the help of an electrocardiogram, various pathologies of the heart can be detected. Will an EKG show a heart attack? Certainly yes.
What determines an electrocardiogram
- Heart rate - heart rate.
- Rhythms of contractions of the heart.
- Heart attack.
- Arrhythmias.
- Hypertrophy of the ventricles.
- Ischemic and cardiac changes.
The most disappointing and serious diagnosis on the electrocardiogram is myocardial infarction. In the diagnosis of heart attacks, the ECG plays an important and even major role. With the help of a cardiogram, a zone of necrosis, localization and depth of lesions of the heart area are revealed. Also, when deciphering the cardiogram tape, it is possible to recognize and distinguish acute myocardial infarction from aneurysms and past scars. Therefore, when passing a medical examination, it is imperative to do a cardiogram, because it is very important for a doctor to know what the ECG will show.
Most often, a heart attack is associated directly with the heart. But it is not so. A heart attack can occur in any organ. It happens (when the tissues of the lungs partially or completely die off, if there is a blockage of the arteries).
There is a cerebral infarction (in other words, ischemic stroke) - the death of brain tissue, which can be caused by thrombosis or rupture of cerebral vessels. With a cerebral infarction, such functions as the gift of speech, physical movements and sensitivity can completely go astray or disappear.
When a person has a heart attack, death or necrosis of living tissue occurs in his body. The body loses tissue or part of an organ, as well as the functions performed by this organ.
Myocardial infarction is the death or ischemic necrosis of areas or areas of the heart muscle itself due to a complete or partial loss of blood supply. Heart muscle cells begin to die approximately 20-30 minutes after blood flow stops. If a person has a myocardial infarction, blood circulation is disturbed. One or more blood vessels fail. Most often, heart attacks occur due to blockage of blood vessels by blood clots (atherosclerotic plaques). The zone of distribution of the infarction depends on the severity of the disruption of the organ, for example, extensive myocardial infarction or microinfarction. Therefore, you should not immediately despair if the ECG shows a heart attack.

It becomes a threat to the work of the entire of cardio-vascular system body and is life threatening. In the modern period, heart attacks are main reason mortality among the population of developed countries of the world.
Heart attack symptoms
- Dizziness.
- Labored breathing.
- Pain in the neck, shoulder, which can radiate to the back, numbness.
- Cold sweat.
- Nausea, full stomach feeling.
- Feeling of constriction in the chest.
- Heartburn.
- Cough.
- Chronic fatigue.
- Loss of appetite.
The main signs of myocardial infarction
- Intense pain in the region of the heart.
- Pain that does not stop after taking nitroglycerin.
- If the duration of the pain is already more than 15 minutes.
Causes of a heart attack
- Atherosclerosis.
- Rheumatism.
- Congenital heart disease.
- Diabetes.
- Smoking, obesity.
- arterial hypertension.
- Vasculitis.
- Increased blood viscosity (thrombosis).
- Previously transferred heart attacks.
- severe spasms coronary artery(for example, when taking cocaine).
- Age changes.
ECG also allows you to identify other diseases, such as tachycardia, arrhythmia, ischemic disorders.
Arrhythmia
What to do if the ECG showed arrhythmia?
An arrhythmia can be characterized by numerous changes in the contraction of the heartbeat.
An arrhythmia is a condition in which there is a violation heart rate and heart rate. More often this pathology is marked by a heartbeat failure; the patient has a rapid, then a slow heartbeat. An increase occurs during inhalation, and a decrease occurs during exhalation.

angina pectoris
If the patient has bouts of pain under the sternum or to the left of it in the region of the left arm, which can last a few seconds, and can last up to 20 minutes, then the ECG will show angina pectoris.
Pain usually increases with weight lifting, heavy physical exertion, when going out into the cold and may disappear at rest. Such pains are reduced within 3-5 minutes when taking nitroglycerin. The patient's skin turns pale and the pulse becomes uneven, which causes interruptions in the work of the heart.

Angina pectoris is one form of the heart. It is often difficult to diagnose angina pectoris, because such abnormalities can also occur with other cardiac pathologies. Angina pectoris can further lead to heart attacks and strokes.
Tachycardia
Many are very worried when they find out that the ECG showed tachycardia.
Tachycardia is an increase at rest. Heart rhythms with tachycardia can reach up to 100-150 beats per minute. Such a pathology can also occur in people, regardless of age, when lifting weights or with increased physical exertion, as well as with strong psycho-emotional arousal.

Still, tachycardia is considered rather not a disease, but a symptom. But it is no less dangerous. If the heart starts beating too fast, it cannot fill with blood, which further leads to a decrease in blood output and a lack of oxygen in the body, as well as the heart muscle itself. If the tachycardia lasts for more than a month, it can lead to further failure of the heart muscle and an increase in the size of the heart.
Symptoms characteristic of tachycardia
- Dizziness, fainting.
- Weakness.
- Dyspnea.
- Increased anxiety.
- Feeling of increased heart rate.
- Heart failure.
- Pain in the chest.
The causes of tachycardia can be: coronary heart disease, various infections, toxic effects, ischemic changes.
Conclusion
Now there are many different heart diseases that can be accompanied by painful and painful symptoms. Before starting their treatment, it is necessary to diagnose, find out the cause of the problem and, if possible, eliminate it.
To date, an electrocardiogram is the only effective method in diagnosing heart pathologies, which is also completely harmless and painless. This method is suitable for everyone - both children and adults, and is also affordable, effective and highly informative, which is very important in modern life.
An electrocardiographic study is quite simple and effective method diagnostics, used by cardiologists around the world to study the activity of the heart muscle. The results of the procedure in the form of graphs and digital symbols, as a rule, are transferred to specialists for further data analysis. However, in the case of, for example, the absence of the right doctor, the patient has a desire to independently decipher the indicators of his heart.
Preliminary interpretation of the ECG requires knowledge of special basic data, which, due to their specificity, are not subject to everyone. In order to make correct calculations ECG of the heart a person who is not related to medicine needs to familiarize himself with the basic principles of processing, which are combined for convenience into appropriate blocks.
Familiarization with the basic elements of a cardiogram
You should know that the interpretation of the ECG is carried out thanks to elementary, logical rules that can be understood even by an ordinary layman. For a more pleasant and calm perception of them, it is recommended to start familiarizing yourself first with the simplest principles of decoding, gradually moving to a more complex level of knowledge.
Ribbon layout
The paper, which reflects data on the functioning of the heart muscle, is a wide ribbon of a soft pink hue with a clear “square” marking. The larger quadrilaterals are formed from 25 small cells, and each of them, in turn, equates to 1 mm. If a large cell is filled with only 16 dots, for convenience, you can draw parallel lines along them and follow similar instructions.
The horizontals of the cells indicate the duration of the heartbeat (sec), and the verticals indicate the voltage of individual ECG segments (mV). 1 mm is 1 second of time (in width) and 1 mV of voltage (in height)! This axiom must be kept in mind throughout the entire period of data analysis, later its importance will become obvious to everyone.
The paper used allows you to correctly analyze the time intervals
teeth and segments
Before moving on to the names of specific departments of the gear graph, it is worth familiarizing yourself with the activity of the heart itself. The muscular organ consists of 4 compartments: the 2 upper ones are called the atria, the 2 lower ones are called the ventricles. Between the ventricle and the atrium in each half of the heart there is a valve - a leaflet responsible for accompanying blood flow in one direction: from top to bottom.
This activity is achieved due to electrical impulses that move through the heart according to the "biological timetable". They are sent to specific segments of the hollow organ using a system of bundles and nodes, which are miniature muscle fibers.
The birth of the impulse occurs in the upper part of the right ventricle - the sinus node. Further, the signal passes into the left ventricle and excitation of the upper parts of the heart is observed, which is recorded by the P wave on the ECG: it looks like a gentle inverted cup.
After the electric charge reaches the atrioventricular node (or AV node), which is located almost at the junction of all 4 pockets of the heart muscle, a small “point” appears on the cardiogram, pointing down - this is the Q wave. Just below the AV node there is the following item the purpose of the impulse is the bundle of His, which is fixed by the highest tooth R among others, which can be represented as a peak or mountain.
Having overcome half of the way, an important signal rushes to the lower part of the heart, through the so-called legs of the bundle of His, outwardly resembling the long tentacles of an octopus that hug the ventricles. The conduction of the impulse along the branched processes of the bundle is reflected in the S wave - a shallow groove at the right foot of R. When the impulse spreads to the ventricles along the legs of the bundle of His, they contract. The last bumpy T wave marks the recovery (rest) of the heart before the next cycle.

Not only cardiologists, but also other specialists can decipher diagnostic indicators.
In front of the 5 main teeth on the ECG, you can see a rectangular protrusion, you should not be afraid of it, since it is a calibration or control signal. Between the teeth there are horizontally directed sections - segments, for example, S-T (from S to T) or P-Q (from P to Q). To independently make an indicative diagnosis, you will need to remember such a concept as the QRS complex - the combination of the Q, R and S teeth, which registers the work of the ventricles.
The teeth that rise above the isometric line are called positive, and those that are located below them are called negative. Therefore, all 5 teeth alternate one after the other: P (positive), Q (negative), R (positive), S (negative) and T (positive).
Leads
Often you can hear the question from people: why are all the ECG graphs different from each other? The answer is relatively simple. Each of the curved lines on the tape reflects the heart readings obtained from 10-12 colored electrodes, which are installed on the limbs and in the chest area. They read data on the heart impulse, located at different distances from the muscle pump, because the graphics on the thermal tape are often different from each other.
Only an experienced specialist can competently write an ECG conclusion, while the patient has the opportunity to consider general information about your health.
Normal indicators of the cardiogram
Now that it has become clear how to decipher the cardiogram of the heart, one should proceed to the direct diagnosis of normal readings. But before getting acquainted with them, it is necessary to evaluate the ECG recording speed (50 mm / s or 25 mm / s), which, as a rule, is automatically printed on paper tape. Then, starting from the result, you can view the norms for the duration of the teeth and segments that are listed in the table (calculations can be carried out using a ruler or checkered markings on the tape):
Among the most significant provisions of the interpretation of the ECG, the following can be mentioned:
- The S-T and P-Q segments should "merge" with the isometric line without going beyond it.
- The depth of the Q wave cannot exceed ¼ of the height of the most slender tooth - R.
- The exact measurements of the S wave have not been confirmed, but it is known that it sometimes reaches a depth of 18–20 mm.
- The T wave should not be higher than R: its maximum value is ½ of the height of R.
Heart rate control is also important. It is necessary to pick up a ruler and measure the length of the segments enclosed between the vertices of R: the results obtained must coincide with each other. To calculate the heart rate (or heart rate), it is worth counting the total number of small cells between the 3 vertices of R and dividing the digital value by 2. Next, you need to apply one of the 2 formulas:
- 60/X*0.02 (at 50mm/s write speed).
- 60/X*0.04 (at 25mm/s write speed).
If the figure is in the range from 59-60 to 90 beats / min, then the heart rate is normal. An increase in this index implies tachycardia, and a clear decrease implies bradycardia. If for a well-formed person a heart rate of more than 95–100 beats per minute is a rather dubious sign, then for children under 5–6 years old this is one of the varieties of the norm.

Each of the teeth and intervals indicates a certain period of time for the work of the heart muscle.
What pathologies can be identified when deciphering the data?
Although the ECG is one of the extremely simple studies in terms of structure, there are still no analogues of such a diagnosis of cardiac abnormalities. The most "popular" diseases recognized by ECG can be found by examining both the description of their characteristic indicators and detailed graphic examples.
This ailment often recorded in adults during the implementation of the ECG, in children it is extremely rare. Among the most common "catalysts" of the disease are the use of drugs and alcohol, chronic stress, hyperthyroidism, etc. PT is distinguished, first of all, by a frequent heartbeat, the indicators of which range from 138-140 to 240-250 beats / min.
Due to the manifestation of such attacks (or paroxysm), both ventricles of the heart do not have the opportunity to fill with blood in time, which weakens the overall blood flow and slows down the delivery of the next portion of oxygen to all parts of the body, including the brain. Tachycardia is characterized by the presence of a modified QRS complex, a mild T wave, and, most importantly, the absence of a distance between T and P. In other words, the groups of teeth on the electrocardiogram are "glued" to each other.

The disease is one of the "invisible killers" and requires immediate contact with a number of specialists, since if it is extremely neglected, it can lead to the death of a person.
Bradycardia
If the previous anomaly implied the absence of the T-P segment, then bradycardia is its antagonist. This disease gives out a significant elongation T-P, indicating weak conduction of the impulse or its incorrect accompaniment through the heart muscle. In patients with bradycardia, an extremely low heart rate index is observed - less than 40-60 bpm. If in people who prefer regular physical activity, a mild manifestation of the disease is the norm, then in the vast majority of other cases, we can talk about the emergence of an extremely serious disease.
If obvious signs of bradycardia are found, a comprehensive examination should be carried out in the near future.
Ischemia
Ischemia is called a harbinger of myocardial infarction, for this reason early detection anomalies contributes to the relief of fatal ailments and, as a result, a favorable outcome. It was previously mentioned that the S-T interval should “comfortably lie” on the isoline, however, its omission in the 1st and AVL leads (up to 2.5 mm) signals precisely about IHD. Sometimes coronary heart disease gives out only the T wave. Normally, it should not exceed ½ of the R height, however, in this case it can either “grow” to the older element or fall below the midline. The remaining teeth are not subject to significant changes.
Flutter and atrial fibrillation
Atrial fibrillation is an abnormal condition of the heart, expressed in a disorderly, chaotic manifestation of electrical impulses in the upper pockets of the heart. It is sometimes not possible to make a qualitative surface analysis in such a case. But knowing what you should pay attention to first of all, you can safely decipher ECG indicators. QRS complexes are not of fundamental importance, since they are often stable, but the gaps between them are key indicators: when they flicker, they look like a series of notches on a hand saw.

Pathologies are clearly distinguishable on the cardiogram
Not so chaotic, large-sized waves between the QRS already indicate atrial flutter, which, unlike flicker, is characterized by a slightly more pronounced heartbeat (up to 400 beats / min). Contractions and excitations of the atria are subject to control to a small extent.
Thickening of the atrial myocardium
Suspicious thickening and stretching of the muscle layer of the myocardium is accompanied by a significant problem with the internal blood flow. At the same time, the atria perform their main function with constant interruptions: the thickened left chamber “pushes” blood into the ventricle with greater force. When trying to read an ECG graph at home, you should focus on the P wave, which reflects the state of the upper heart.
If it is a kind of dome with two bulges, most likely the patient is suffering from the disease in question. Since thickening of the myocardium in the absence of qualified medical intervention for a long time provokes a stroke or heart attack, it is necessary to make an appointment with a cardiologist as soon as possible, providing a detailed description of uncomfortable symptoms, if any.
Extrasystole
It is possible to decipher the ECG with the "first signs" of extrasystole if there is knowledge about the special indicators of a special manifestation of arrhythmia. By carefully examining such a graph, the patient can detect unusual abnormal jumps that vaguely resemble QRS complexes - extrasystoles. They occur in any area of the ECG, they are often followed by a compensatory pause, allowing the heart muscle to “rest” before starting a new cycle of excitations and contractions.
Extrasystole in medical practice is often diagnosed in healthy people. In the vast majority of cases, it does not affect the usual course of life and is not associated with serious illnesses. However, when establishing an arrhythmia, you should play it safe by contacting specialists.
With atrioventricular heart block, an expansion of the gap between the P waves of the same name is observed, in addition, they can occur at the time of analyzing the ECG conclusion much more often than QRS complexes. The registration of such a pattern indicates a low conductivity of the impulse from the upper chambers of the heart to the ventricles.

If the disease progresses, the electrocardiogram changes: now the QRS “drops out” from the general row of P waves in some intervals
Blockade of the legs of the bundle of His
The failure of such an element of the conduction system as the bundle of His should in no case be ignored, since it is located in close proximity to the Myocardium. The pathological focus in advanced cases tends to "transfer" to one of the most important parts of the heart. Decipher the ECG yourself if there is an extremely unpleasant disease it is quite possible, you just have to carefully examine the highest prong on the thermal tape. If it forms not a “slender” letter L, but a deformed M, this means that the bundle of His has been attacked.
The defeat of its left leg, which passes the impulse into the left ventricle, entails the complete disappearance of the S wave. And the place of contact of the two vertices of the split R will be located above the isoline. Cardiographic image of attenuation right leg beam is similar to the previous one, only the junction point of the already marked vertices of the R wave is under the midline. T is negative in both cases.
myocardial infarction
The myocardium is a fragment of the densest and thickest layer of the heart muscle, which in last years subjected to various ailments. The most dangerous among them is necrosis or myocardial infarction. When deciphering electrocardiography, it is quite distinguishable from other types of diseases. If the P wave, which registers the good condition of the 2 atria, is not deformed, then the remaining segments of the ECG have undergone significant changes. So, a pointed Q wave can “pierce” the isoline plane, and T can be transformed into a negative tooth.
The most telling sign of a heart attack is abnormal elevation R-T. There is a mnemonic rule that allows you to remember its exact appearance. If, when examining this area, one can imagine the left, ascending side of R in the form of a rack tilted to the right, on which a flag flies, then we are really talking about myocardial necrosis.

The disease is diagnosed both in the acute phase and after the attack subsides.
ventricular fibrillation
Otherwise, an extremely serious illness is called atrial fibrillation. A distinctive feature of this pathological phenomenon is considered to be the destructive activity of the conductive bundles and nodes, indicating an uncontrolled contraction of all 4 chambers of the muscle pump. Reading the results of an ECG and recognizing ventricular fibrillation is not at all difficult: on a checkered tape, it appears as a series of chaotic waves and hollows, the parameters of which cannot be correlated with classical indicators. In none of the segments can you see at least one familiar complex.
If a patient with atrial fibrillation is not given premature medical care he will soon die.
WPW syndrome
When, in the complex of classical pathways for conducting an electrical impulse, an abnormal Kent bundle is unexpectedly formed, located in the “comfortable cradle” of the left or right atrium, we can confidently speak of such a pathology as WPW syndrome. As soon as the impulses begin to move along the unnatural cardiac highway, the rhythm of the muscle goes astray. The “correct” conductive fibers cannot fully supply the atria with blood, because the impulses preferred more short cut to complete the functional cycle.
The ECG in SVC syndrome is distinguished by the appearance of a microwave at the left foot of the R wave, a slight widening of the QRS complex, and, of course, a significant reduction interval P-Q. Since the decoding of the cardiogram of a heart that has undergone WPW is not always effective, HM comes to the aid of medical personnel - the Holter method for diagnosing an ailment. It involves the round-the-clock wearing on the body of a compact device with attached to skin sensors.
Long-term monitoring provides a better result with a reliable diagnosis. In order to “catch” the anomaly localized in the heart in a timely manner, it is recommended to visit the ECG room at least once a year. If regular medical monitoring of the treatment of cardiovascular disease is necessary, more frequent measurements of cardiac activity may be required.
ECG (electrocardiography, or simply, a cardiogram) is the main method for studying cardiac activity. The method is so simple, convenient, and, at the same time, informative that it is used everywhere. In addition, the ECG is absolutely safe, and there are no contraindications to it.
Therefore, it is used not only for diagnosing cardiovascular diseases, but also as a preventive measure during planned medical examinations, before sports competitions. In addition, an ECG is recorded to determine suitability for certain professions associated with heavy physical exertion.
Our heart contracts under the action of impulses that pass through the conduction system of the heart. Each pulse represents an electrical current. This current originates at the site of impulse generation in the sinus node, and then goes to the atria and ventricles. Under the action of the impulse, contraction (systole) and relaxation (diastole) of the atria and ventricles occur.
Moreover, systoles and diastoles occur in a strict sequence - first in the atria (in the right atrium a little earlier), and then in the ventricles. This is the only way to ensure normal hemodynamics (blood circulation) with a full supply of blood to organs and tissues.
Electric currents in the conduction system of the heart create an electric and magnetic field around them. One of the characteristics of this field is the electric potential. With abnormal contractions and inadequate hemodynamics, the magnitude of the potentials will differ from the potentials characteristic of the heart contractions of a healthy heart. In any case, both in the norm and in pathology, the electrical potentials are negligible.
But tissues have electrical conductivity, and therefore the electric field of a beating heart spreads throughout the body, and the potentials can be recorded on the surface of the body. All that is needed for this is a highly sensitive apparatus equipped with sensors or electrodes. If using this device, called an electrocardiograph, to register electrical potentials corresponding to the impulses of the conducting system, then it is possible to judge the work of the heart and diagnose violations of its work.
This idea formed the basis of the corresponding concept developed by the Dutch physiologist Einthoven. At the end of the XIX century. this scientist formulated the basic principles of the ECG and created the first cardiograph. In a simplified form, an electrocardiograph consists of electrodes, a galvanometer, an amplification system, lead switches, and a recording device. Electric potentials are perceived by electrodes, which are superimposed on various parts of the body. The choice of assignment is carried out by means of the switch of the device.
Since the electrical potentials are negligible, they are first amplified and then fed to the galvanometer, and from there, in turn, to the recording device. This device is an ink recorder and paper tape. Already at the beginning of the 20th century. Einthoven was the first to use ECG for diagnostic purposes, for which he was awarded the Nobel Prize.
ECG Einthoven triangle
According to Einthoven's theory, the human heart, located in chest offset to the left, located in the center of a kind of triangle. The vertices of this triangle, which is called Einthoven's triangle, are formed by three limbs - the right hand, the left hand, and the left foot. Einthoven proposed to register the potential difference between the electrodes applied to the limbs.
The potential difference is determined in three leads, which are called standard, and denoted by Roman numerals. These leads are the sides of Einthoven's triangle. In this case, depending on the lead in which the ECG is recorded, the same electrode can be active, positive (+), or negative (-):
- Left hand (+) - right hand (-)
- Right arm (-) - left leg (+)
- Left hand (-) - left leg (+)
Rice. 1. Einthoven's triangle.
A little later, it was proposed to record enhanced unipolar leads from the extremities - the vertices of the Eithoven triangle. These enhanced leads are designated by the English abbreviations aV (augmented voltage - enhanced potential).
aVL (left) - left hand;
aVR (right) - right hand;
aVF (foot) - left foot.
In reinforced unipolar leads, the potential difference between the limb on which the active electrode is applied and the average potential of the other two limbs is determined.
In the middle of the XX century. The ECG was supplemented by Wilson, who, in addition to standard and unipolar leads, proposed recording the electrical activity of the heart from unipolar chest leads. These leads are denoted by the letter V. In an ECG study, six unipolar leads located on the anterior surface of the chest are used.
Since cardiac pathology, as a rule, affects the left ventricle of the heart, most chest leads V are located in the left half of the chest.

Rice. 2.
V 1 - fourth intercostal space at the right edge of the sternum;
V 2 - fourth intercostal space at the left edge of the sternum;
V 3 - the middle between V 1 and V 2;
V 4 - fifth intercostal space along the midclavicular line;
V 5 - horizontally along the anterior axillary line at the level of V 4;
V 6 - horizontally along the midaxillary line at the level of V 4.
These 12 leads (3 standard + 3 unipolar limb + 6 chest) are mandatory. They are recorded and evaluated in all cases of ECG for diagnostic or prophylactic purposes.
In addition, there are a number of additional leads. They are recorded rarely and for certain indications, for example, when it is necessary to clarify the localization of myocardial infarction, to diagnose hypertrophy of the right ventricle, auricles, etc. Additional ECG leads include chest:
V 7 - at the level of V 4 -V 6 along the posterior axillary line;
V 8 - at the level of V 4 -V 6 along the scapular line;
V 9 - at the level of V 4 -V 6 along the paravertebral (paravertebral) line.
In rare cases, to diagnose changes in the upper parts of the heart, chest electrodes can be located 1-2 intercostal spaces higher than usual. In this case, V 1 , V 2 are denoted, where the superscript reflects how many intercostal spaces the electrode is located above.
Sometimes, to diagnose changes in the right parts of the heart, chest electrodes are placed on the right half of the chest at points that are symmetrical to those in the standard method of recording chest leads in the left half of the chest. In the designation of such leads, the letter R is used, which means right, right - B 3 R, B 4 R.
Cardiologists sometimes resort to bipolar leads, once proposed by the German scientist Neb. The principle of registration of leads in the Sky is approximately the same as the registration of standard leads I, II, III. But in order to form a triangle, the electrodes are applied not to the limbs, but to the chest.
The electrode from the right hand of the hand is placed in the second intercostal space at the right edge of the sternum, from the left hand - along the posterior axillary line at the level of the vane of the heart, and from the left leg - directly to the projection point of the vane of the heart, corresponding to V 4 . Between these points, three leads are recorded, which are denoted by the Latin letters D, A, I:
D (dorsalis) - posterior lead, corresponds to standard lead I, resembles V 7 ;
A (anterior) - anterior lead, corresponds to standard lead II, resembles V 5 ;
I (inferior) - inferior lead, corresponds to the standard lead III, is similar to V 2 .
For the diagnosis of posterior basal forms of infarction, Slopak leads are recorded, denoted by the letter S. When registering Slopak leads, the electrode applied to left hand, set along the left posterior axillary line at the level of the apical impulse, and the electrode from the right hand is moved alternately to four points:
S 1 - at the left edge of the sternum;
S 2 - along the midclavicular line;
S 3 - in the middle between C 2 and C 4;
S 4 - along the anterior axillary line.
On rare occasions, for ECG diagnostics resort to precordial mapping, when 35 electrodes in 5 rows of 7 in each are located on the left anterolateral surface of the chest. Sometimes electrodes are placed in the epigastric region, advanced into the esophagus at a distance of 30-50 cm from the incisors, and even inserted into the cavity of the heart chambers when probing it through large vessels. But all these specific ECG recording methods are carried out only in specialized centers with the necessary equipment and qualified doctors.
ECG technique
In a planned manner, ECG recording is carried out in a specialized room equipped with an electrocardiograph. In some modern cardiographs, instead of the usual ink recorder, a thermal printing mechanism is used, which, with the help of heat, burns the cardiogram curve onto paper. But in this case, a special paper or thermal paper is needed for the cardiogram. For clarity and convenience of calculating ECG parameters in cardiographs, graph paper is used.
In cardiographs of the latest modifications, the ECG is displayed on the monitor screen, decrypted using the supplied software, and not only printed on paper, but also stored on a digital medium (disk, flash drive). Despite all these improvements, the principle of the device of the ECG recording cardiograph has not changed much since the time it was developed by Einthoven.
Most modern electrocardiographs are multichannel. Unlike traditional single-channel devices, they register not one, but several leads at once. In 3-channel devices, first standard I, II, III are recorded, then reinforced unipolar limb leads aVL, aVR, aVF, and then chest leads - V 1-3 and V 4-6. In 6-channel electrocardiographs, standard and unipolar limb leads are first recorded, and then all chest leads.
The room in which the recording is carried out must be away from sources of electromagnetic fields, x-ray radiation. Therefore, the ECG room should not be placed in close proximity to the X-ray room, rooms where physiotherapy procedures are performed, as well as electric motors, power panels, cables, etc.
Special preparation before recording an ECG is not carried out. It is desirable that the patient was rested and slept. Previous physical and psycho-emotional stresses can affect the results and are therefore undesirable. Sometimes food intake can also affect the results. Therefore, the ECG is recorded on an empty stomach, not earlier than 2 hours after eating.
During the recording of the ECG, the subject lies on a flat hard surface (on the couch) in a relaxed state. Places for applying electrodes should be free from clothing.
Therefore, you need to undress to the waist, legs and feet free from clothes and shoes. Electrodes are applied to internal surfaces lower thirds shins and feet (inner surface of the wrist and ankle joints). These electrodes have the form of plates and are designed to register standard leads and unipolar leads from the extremities. These same electrodes can look like bracelets or clothespins.
Each limb has its own electrode. To avoid errors and confusion, the electrodes or wires through which they are connected to the device are color-coded:
- To right hand- red;
- To the left hand - yellow;
- To the left leg - green;
- To right leg- black.
Why do you need a black electrode? After all, the right leg is not included in the Einthoven triangle, and readings are not taken from it. The black electrode is for grounding. According to the basic safety requirements, all electrical equipment, incl. and electrocardiographs must be grounded.
To do this, ECG rooms are equipped with a ground loop. And if the ECG is recorded in a non-specialized room, for example, at home by ambulance workers, the device is grounded to a central heating battery or to a water pipe. To do this, there is a special wire with a fixing clip at the end.
Electrodes for registration of chest leads have the form of a pear-suction cup, and are equipped with a wire white color. If the device is single-channel, there is only one suction cup, and it is moved to the required points on the chest.
There are six of these suction cups in multichannel devices, and they are also color-coded:
V 1 - red;
V 2 - yellow;
V 3 - green;
V 4 - brown;
V 5 - black;
V 6 - purple or blue.
It is important that all electrodes fit snugly against the skin. The skin itself should be clean, devoid of sebaceous fat and sweat secretions. Otherwise, the quality of the electrocardiogram may deteriorate. Between the skin and the electrode there are induction currents, or simply, pickup. Quite often, a tip-off occurs in men with thick hair on the chest and on the limbs. Therefore, here it is especially necessary to ensure that the contact between the skin and the electrode is not disturbed. The pickup sharply degrades the quality of the electrocardiogram, on which small teeth are displayed instead of a flat line.

Rice. 3. Flooding currents.
Therefore, the place where the electrodes are applied is recommended to be degreased with alcohol, moistened with soapy water or conductive gel. For electrodes from the extremities, gauze wipes moistened with saline are also suitable. However, it should be borne in mind that saline dries quickly, and contact may be broken.
Before recording, it is necessary to check the calibration of the device. For this, it has a special button - the so-called. control millivolt. This value reflects the height of the tooth at a potential difference of 1 millivolt (1 mV). In electrocardiography, the value of the control millivolt is 1 cm. This means that with a difference in electrical potentials of 1 mV, the height (or depth) wave ECG equal to 1 cm.

Rice. 4. Each ECG recording must be preceded by a control millivolt check.
Recording of electrocardiograms is carried out at a tape speed of 10 to 100 mm/s. True, extreme values are used very rarely. Basically, the cardiogram is recorded at a speed of 25 or 50 mm / s. Moreover, the last value, 50 mm / s, is standard, and most often used. A speed of 25 mm/h is used where the greatest number of heart contractions must be recorded. After all, the lower the speed of the tape, the greater the number of contractions of the heart it displays per unit of time.

Rice. 5. The same ECG recorded at 50 mm/s and 25 mm/s.
The ECG is recorded with quiet breathing. In this case, the subject should not talk, sneeze, cough, laugh, make sudden movements. When registering the III standard lead, a deep breath with a short breath hold may be required. This is done in order to distinguish functional changes, which are quite often found in this lead, from pathological ones.
The section of the cardiogram with teeth corresponding to the systole and diastole of the heart is called the cardiac cycle. Usually, 4-5 cardiac cycles are recorded in each lead. In most cases, this is sufficient. However, in case of cardiac arrhythmias, if myocardial infarction is suspected, recording up to 8-10 cycles may be required. To switch from one lead to another, the nurse uses a special switch.
At the end of the recording, the subject is released from the electrodes, and the tape is signed - at the very beginning, the full name is indicated. and age. Sometimes, to detail the pathology or determine physical endurance, an ECG is performed against the background of medication or physical exertion. Drug tests are carried out with various drugs - atropine, chimes, potassium chloride, beta-blockers. Physical activity is carried out on an exercise bike (veloergometry), with walking on a treadmill, or walking for certain distances. For completeness of information, the ECG is recorded before and after exercise, as well as directly during bicycle ergometry.
Many negative changes in the work of the heart, such as rhythm disturbances, are transient and may not be detected during an ECG recording, even with a large number of leads. In these cases, Holter monitoring is performed - an ECG is recorded according to Holter in continuous mode during the day. A portable recorder equipped with electrodes is attached to the patient's body. Then the patient goes home, where he leads the usual mode for himself. After a day, the recording device is removed and the available data is decoded.
A normal ECG looks something like this:
Rice. 6. Tape with ECG
All deviations in the cardiogram from midline(isolines) are called teeth. The teeth deviated upward from the isoline are considered to be positive, downward - negative. The gap between the teeth is called a segment, and the tooth and its corresponding segment are called the interval. Before finding out what a particular wave, segment or interval is, it is worth briefly dwelling on the principle of forming an ECG curve.
Normally, the heart impulse originates in the sinoatrial (sinus) node of the right atrium. Then it spreads to the atria - first the right, then the left. After that, the impulse is sent to the atrioventricular node (atrioventricular or AV junction), and further along the bundle of His. Branches of the bundle of His or legs (right, left anterior and left posterior) end with Purkinje fibers. From these fibers, the impulse propagates directly to the myocardium, leading to its contraction - systole, which is replaced by relaxation - diastole.
The passage of an impulse along nerve fiber and the subsequent contraction of the cardiomyocyte is a complex electromechanical process during which the values of electrical potentials on both sides of the fiber membrane change. The difference between these potentials is called the transmembrane potential (TMP). This difference is due to the unequal permeability of the membrane for potassium and sodium ions. Potassium is more inside the cell, sodium - outside it. With the passage of the pulse, this permeability changes. Similarly, the ratio of intracellular potassium and sodium, and TMP changes.
When the excitatory impulse passes, TMP inside the cell rises. In this case, the isoline shifts upward, forming the ascending part of the tooth. This process is called depolarization. Then, after the passage of the pulse, the TMT tries to take the initial value. However, the permeability of the membrane for sodium and potassium does not immediately return to normal, and takes some time.
This process, called repolarization, on the ECG is manifested by a downward deviation of the isoline and the formation of a negative tooth. Then the membrane polarization takes the initial value (TMP) of rest, and the ECG again takes on the character of an isoline. This corresponds to the diastolic phase of the heart. It is noteworthy that the same tooth can look both positive and negative. Everything depends on the projection, i.e. the lead in which it registers.
Components of an ECG
ECG waves are usually denoted by Latin capital letters, starting with the letter R.
Rice. 7. Teeth, segments and intervals of the ECG.
The parameters of the teeth are the direction (positive, negative, two-phase), as well as the height and width. Since the height of the tooth corresponds to the change in potential, it is measured in mV. As already mentioned, a height of 1 cm on the tape corresponds to a potential deviation of 1 mV (control millivolt). The width of a tooth, segment or interval corresponds to the duration of the phase of a certain cycle. This is a temporary value, and it is customary to denote it not in millimeters, but in milliseconds (ms).
When the tape moves at a speed of 50 mm / s, each millimeter on paper corresponds to 0.02 s, 5 mm to 0.1 ms, and 1 cm to 0.2 ms. It's very simple: if 1 cm or 10 mm (distance) is divided by 50 mm/s (speed), then we get 0.2 ms (time).
Tooth R. Displays the spread of excitation through the atria. In most leads, it is positive, and its height is 0.25 mV, and its width is 0.1 ms. Moreover, the initial part of the wave corresponds to the passage of the impulse through the right ventricle (since it is excited earlier), and the final part - through the left. The P wave may be inverted or biphasic in leads III, aVL, V 1 , and V 2 .
Interval P-Q (orP-R)- the distance from the beginning of the P wave to the beginning of the next wave - Q or R. This interval corresponds to the depolarization of the atria and the passage of the impulse through the AV junction, and further along the bundle of His and its legs. The value of the interval depends on the heart rate (HR) - the higher it is, the shorter the interval. Normal values are in the range of 0.12 - 0.2 ms. A wide interval indicates a slowdown in atrioventricular conduction.
Complex QRS. If P represents atrial work, then the next waves, Q, R, S and T, represent ventricular function, and correspond to different phases of depolarization and repolarization. The combination of QRS waves is called the ventricular QRS complex. Normally, its width should be no more than 0.1 ms. Excess indicates a violation of intraventricular conduction.
Prong Q. Corresponds to depolarization of the interventricular septum. This tooth is always negative. Normally, the width of this wave does not exceed 0.3 ms, and its height is no more than ¼ of the R wave following it in the same lead. The only exception is lead aVR, where a deep Q wave is recorded. In other leads, a deep and widened Q wave (in medical slang - kuishche) may indicate a serious pathology of the heart - an acute myocardial infarction or scarring after a heart attack. Although other reasons are possible - deviations of the electrical axis during hypertrophy of the heart chambers, positional changes, blockade of the legs of the bundle of His.
ProngR .Displays the spread of excitation through the myocardium of both ventricles. This wave is positive, and its height does not exceed 20 mm in the limb leads and 25 mm in the chest leads. The height of the R wave is not the same in different leads. Normally, in lead II, it is the largest. In ore allotments V 1 and V 2 it is low (because of this, it is often denoted by the letter r), then it increases in V 3 and V 4, and again decreases in V 5 and V 6. In the absence of an R wave, the complex takes the form of a QS, which may indicate a transmural or cicatricial myocardial infarction.
Prong S. Displays the passage of the impulse along the lower (basal) part of the ventricles and the interventricular septum. This is a negative prong, and its depth varies widely, but should not exceed 25 mm. In some leads, the S wave may be absent.
T wave. The final section of the ECG complex, showing the phase of rapid ventricular repolarization. In most leads, this wave is positive, but it can also be negative in V 1 , V 2 , aVF. The height of the positive teeth directly depends on the height of the R wave in the same lead - the higher the R, the higher the T. The causes of the negative T wave are diverse - small-focal myocardial infarction, dyshormonal disorders, previous meals, changes in the electrolyte composition of the blood, and much more. The width of the T waves usually does not exceed 0.25 ms.
Segment S-T- the distance from the end of the ventricular QRS complex to the beginning of the T wave, corresponding to the complete coverage of the excitation of the ventricles. Normally, this segment is located on the isoline or deviates slightly from it - no more than 1-2 mm. Large S-T deviations indicate a severe pathology - a violation of the blood supply (ischemia) of the myocardium, which can turn into a heart attack. Other, less serious causes are also possible - early diastolic depolarization, a purely functional and reversible disorder, mainly in young men under 40 years of age.
Interval Q-T- the distance from the beginning of the Q wave to the T wave. Corresponds to ventricular systole. Value the interval depends on the heart rate - the faster the heart beats, the shorter the interval.
ProngU . An unstable positive wave, which is recorded after the T wave after 0.02-0.04 s. The origin of this tooth is not fully understood, and it has no diagnostic value.
ECG interpretation
Heart rhythm . Depending on the source of impulse generation of the conduction system, sinus rhythm, rhythm from the AV junction, and idioventricular rhythm are distinguished. Of these three options, only sinus rhythm is normal, physiological, and the remaining two options indicate serious disorders in the conduction system of the heart.
A distinctive feature of sinus rhythm is the presence of atrial P waves - after all, the sinus node is located in the right atrium. With a rhythm from the AV junction, the P wave will overlap the QRS complex (while it is not visible, or follow it. In idioventricular rhythm, the source of the pacemaker is in the ventricles. At the same time, widened deformed QRS complexes are recorded on the ECG.
heart rate. It is calculated by the size of the gaps between the R waves of neighboring complexes. Each complex corresponds heart contraction. Calculating heart rate is easy. You need to divide 60 by the R-R interval, expressed in seconds. For example, the interval R-R equals 50 mm or 5 cm. At a tape speed of 50 m / s, it is equal to 1 s. Divide 60 by 1 and you get 60 heartbeats per minute.
Normal heart rate is in the range of 60-80 beats / min. Exceeding this indicator indicates an increase in heart rate - about tachycardia, and a decrease - about a slowdown, about bradycardia. With a normal rhythm R-R gaps on the ECG should be the same, or approximately the same. Slight difference allowed R-R values, but not more than 0.4 ms, i.e. 2 cm. This difference is typical for respiratory arrhythmias. This is a physiological phenomenon that is often observed in young people. With respiratory arrhythmia, there is a slight decrease in heart rate at the height of inspiration.
alpha angle. This angle reflects the total electrical axis of the heart (EOS) - the general directing vector of electrical potentials in each fiber of the conduction system of the heart. In most cases, the directions of the electrical and anatomical axis of the heart coincide. The alpha angle is determined by the six-axis Bailey coordinate system, where standard and unipolar limb leads are used as axes.

Rice. 8. Six-axis coordinate system according to Bailey.
The alpha angle is determined between the axis of the first lead and the axis where the largest R wave is recorded. Normally, this angle ranges from 0 to 90 0 . In this case, the normal position of the EOS is from 30 0 to 69 0, vertical - from 70 0 to 90 0, and horizontal - from 0 to 29 0. An angle of 91 or more indicates EOS deviation to the right, and negative values of this angle indicate EOS deviation to the left.
In most cases, a six-axis coordinate system is not used to determine the EOS, but they do it approximately, according to the value of R in standard leads. In the normal position of the EOS, the height R is the largest in lead II, and the smallest in lead III.
With the help of an ECG, various violations of the rhythm and conduction of the heart, hypertrophy of the chambers of the heart (mainly the left ventricle), and much more are diagnosed. ECG plays a key role in the diagnosis of myocardial infarction. According to the cardiogram, one can easily determine the duration and prevalence of a heart attack. Localization is judged by the leads in which pathological changes are found:
I - anterior wall of the left ventricle;
II, aVL, V 5 , V 6 - anterolateral, lateral wall of the left ventricle;
V 1 -V 3 - interventricular septum;
V 4 - the apex of the heart;
III, aVF – posterior diaphragmatic wall of the left ventricle.
ECG is also used to diagnose cardiac arrest and assess the effectiveness of resuscitation. When the heart stops, all electrical activity stops, and a solid isoline is visible on the cardiogram. If resuscitation measures ( indirect massage heart, drug administration) were successful, the ECG again shows the teeth corresponding to the work of the atria and ventricles.
And if the patient looks and smiles, and there is an isoline on the ECG, then two options are possible - either errors in the ECG recording technique, or a malfunction of the device. The ECG registration is carried out by a nurse, the interpretation of the data obtained is carried out by a cardiologist or a doctor of functional diagnostics. Although a doctor of any specialty is obliged to navigate in matters of ECG diagnostics.
Registration of an electrocardiogram is a method of studying electrical signals generated during the activity of the muscles of the heart. To record electrocardiogram data, 10 electrodes are used: 1 zero on the right leg, 3 standard ones from the extremities and 6 in the heart area.
The result of the removal of electrical indicators, the work of various departments of the body, is the creation of an electrocardiogram. 
Its parameters are recorded on a special roll paper. Paper movement speed is available in 3 options:
- 25 mm.sec;
- 50 mm.sec;
- 100 mm.sec;
There are electronic sensors that can record ECG parameters on HDD system unit and, if necessary, display this data on the monitor or print it on the required paper sizes.
Interpretation of the recorded electrocardiogram.
The specialist cardiologist gives the result of the analysis of the parameters of the electrocardiogram. The doctor deciphers the record by establishing the duration of the intervals between the various elements of the recorded indicators. An explanation of the features of the electrocardiogram contains many points:

Normal ECG.
Consideration of a standard cardiogram of the heart is represented by the following indicators:

Electrocardiogram in case of myocardial infarction.
Myocardial infarction occurs due to an exacerbation of coronary disease, when the internal cavity of the coronary artery of the heart muscle is significantly narrowed. If this violation is not eliminated within 15 - 20 minutes, the death of the muscle cells of the heart, which receive oxygen and nutrients from this artery, occurs. This circumstance creates significant disturbances in the functioning of the heart and is a severe and serious threat to life. In the event of a heart attack of the heart, an electrocardiogram will help identify the site of necrosis. The specified cardiogram contains markedly manifested deviations in the electrical signals of the heart muscle:

Heart rhythm disorder.
A disorder in the rhythm of contraction of the heart muscles is detected when shifts appear on the electrocardiogram:

Hypertrophy of the heart.

An increase in the volume of the heart muscles is an adaptation of the body to new conditions of functioning. The changes that appear on the electrocardiogram are determined by a high bioelectric force, a characteristic muscle area, a delay in the movement of bioelectric impulses in its thickness, the appearance of signs oxygen starvation.
Conclusion.
Electrocardiographic indicators of cardiac pathology are diverse. Reading them is a complex activity that requires special training and improvement of practical skills. A specialist characterizing an ECG needs to know the basic principles of the physiology of the heart, various versions of cardiograms. He needs to have skills in the ability to determine anomalies in the activity of the heart. Calculate impact medicines and other factors, the occurrence of differences in the structure of the teeth and intervals of the ECG. Therefore, the interpretation of the electrocardiogram should be entrusted to a specialist who has encountered in his practice with various options for shortcomings in the work of the heart.
You may also be interested
Pathology of the cardiovascular system is one of the most common problems affecting people of all ages. Timely treatment and diagnostics of the circulatory system can significantly reduce the risk of developing dangerous diseases.
To date, the most effective and easily accessible method of studying the work of the heart is an electrocardiogram.
When examining the results of the examination of the patient, doctors pay attention to such components of the ECG as:
- teeth;
- intervals;
- Segments.
Not only their presence or absence is assessed, but also their height, duration, location, direction and sequence.
There are strict normal parameters for each line on the ECG tape, the slightest deviation from which may indicate violations in the work of the heart.
ECG analysis
The entire set of ECG lines is examined and measured mathematically, after which the doctor can determine some parameters of the heart muscle and its conduction system: heart rate, heart rate, pacemaker, conduction, electrical axis of the heart.
To date, all these indicators are investigated by high-precision electrocardiographs.
Sinus rhythm of the heart
This is a parameter that reflects the rhythm of heart contractions that occur under the influence of the sinus node (normal). It shows the coherence of the work of all parts of the heart, the sequence of processes of tension and relaxation of the heart muscle.
The rhythm is very easy to identify by the tallest R waves: if the distance between them is the same throughout the entire recording or deviates by no more than 10%, then the patient does not suffer from arrhythmia.
heart rate
The number of beats per minute can be determined not only by counting the pulse, but also by the ECG. To do this, you need to know the speed at which the ECG was recorded (usually 25, 50 or 100mm / s), as well as the distance between the highest teeth (from one peak to another).
By multiplying the recording time of one mm by length of segment R-R you can get your heart rate. Normally, its performance ranges from 60 to 80 beats per minute.

Source of excitation
The autonomic nervous system of the heart is designed in such a way that the process of contraction depends on the accumulation nerve cells in one of the areas of the heart. Normally, this is the sinus node, the impulses from which diverge throughout the nervous system of the heart.
In some cases, other nodes (atrial, ventricular, atrioventricular) can take on the role of the pacemaker. This can be determined by examining the P wave is inconspicuous, located just above the isoline.
You can read detailed and comprehensive information about the symptoms of cardiosclerosis of the heart.
Conductivity
This is a criterion showing the process of momentum transfer. Normally, impulses are transmitted sequentially from one pacemaker to another, without changing the order.
Electric axle
An indicator based on the process of excitation of the ventricles. Mathematical analysis of Q, R, S waves in leads I and III allows you to calculate a certain resulting vector of their excitation. This is necessary to establish the functioning of the branches of the His bundle.
The obtained angle of inclination of the axis of the heart is estimated by the value: 50-70° normal, 70-90° deviation to the right, 50-0° deviation to the left.
In cases where there is a tilt of more than 90° or more than -30°, there is a serious malfunction in the bundle of His.
Teeth, segments and intervals
Teeth - ECG sections lying above the isoline, their meaning is as follows:
- P- reflects the processes of contraction and relaxation of the atria.
- Q, S- reflect the processes of excitation of the interventricular septum.
- R- the process of excitation of the ventricles.
- T- the process of relaxation of the ventricles.
Intervals are sections of the ECG lying on the isoline.
- PQ- reflects the propagation time of the impulse from the atria to the ventricles.
Segments - sections of the ECG, including an interval and a wave.
- QRST- the duration of the contraction of the ventricles.
- ST- the time of complete excitation of the ventricles.
- TP is the time of electrical diastole of the heart.

Norm in men and women
The decoding of the ECG of the heart and the norms of indicators in adults are presented in this table:

Healthy Childhood Outcomes
Deciphering the results of ECG measurements in children and their norm in this table:

Dangerous diagnoses
What dangerous conditions can be determined by the ECG readings during decoding?
Extrasystole
This phenomenon characterized by irregular heartbeat. A person feels a temporary increase in the frequency of contractions, followed by a pause. It is associated with the activation of other pacemakers, sending along with the sinus node an additional burst of impulses, which leads to an extraordinary contraction.
If extrasystoles appear no more than 5 times per hour, then they cannot cause significant harm to health.
Arrhythmia
Characterized change in the frequency of sinus rhythm when pulses arrive at different frequencies. Only 30% of these arrhythmias require treatment, because can lead to more serious illnesses.
In other cases, this may be a manifestation of physical activity, a change in hormonal levels, the result of a fever and does not threaten health.

Bradycardia
It occurs when the sinus node is weakened, unable to generate impulses with the proper frequency, as a result of which the heart rate also slows down, up to 30-45 beats per minute.
Tachycardia
The opposite phenomenon, characterized by an increase in heart rate over 90 beats per minute. In some cases, temporary tachycardia occurs under the influence of strong physical exertion and emotional stress, as well as during illnesses associated with fever.

Conduction disorder
In addition to the sinus node, there are other underlying pacemakers of the second and third orders. Normally, they conduct impulses from the first-order pacemaker. But if their functions weaken, a person may feel weakness, dizziness caused by depression of the heart.
It is also possible to lower blood pressure, because. the ventricles will contract less frequently or arrhythmically.
Many factors can lead to disruption in the work of the heart muscle itself. Tumors develop, muscle nutrition is disrupted, and depolarization processes fail. Most of these pathologies require serious treatment.
Why there might be differences in performance
In some cases, when re-analyzing the ECG, deviations from previously obtained results are revealed. With what it can be connected?
- different time of day. Usually, an ECG is recommended to be done in the morning or afternoon, when the body has not yet had time to be influenced by stress factors.
- Loads. It is very important that the patient is calm while recording the ECG. The release of hormones can increase heart rate and distort performance. In addition, before the examination, it is also not recommended to engage in heavy physical labor.
- meal. Digestive processes affect blood circulation, and alcohol, tobacco and caffeine can affect heart rate and pressure.
- electrodes. Improper overlap or accidental shifting can seriously change the performance. Therefore, it is important not to move during the recording and degrease the skin in the area where the electrodes are applied (the use of creams and other skin products before the examination is highly undesirable).
- Background. Sometimes other devices can interfere with the operation of the electrocardiograph.

Additional examination methods
Halter
Method long-term study of the work of the heart, made possible by a portable compact tape recorder that is capable of recording results on magnetic tape. The method is especially good when it is necessary to investigate recurrent pathologies, their frequency and time of occurrence.

Treadmill
Unlike a normal resting ECG, this method based on results analysis after physical activity . It is most commonly used for risk assessment. possible pathologies not detected on a standard ECG, as well as when prescribing a course of rehabilitation to patients who have had a heart attack.
Phonocardiography
 Allows analyze heart sounds and murmurs. Their duration, frequency and time of occurrence correlate with the phases of cardiac activity, which makes it possible to assess the functioning of the valves, the risks of developing endocarditis and rheumatic heart disease.
Allows analyze heart sounds and murmurs. Their duration, frequency and time of occurrence correlate with the phases of cardiac activity, which makes it possible to assess the functioning of the valves, the risks of developing endocarditis and rheumatic heart disease.
A standard ECG is a graphic representation of the work of all parts of the heart. Its accuracy can be affected by many factors, so doctor's advice should be followed.
The examination reveals most of the pathologies of the cardiovascular system, however, additional tests may be required for an accurate diagnosis.
Finally, we suggest watching a video course on decoding “ECG for everyone”:



